

No Morning Wood? Consider It the Canary in the CVD Coal Mine.
What's causing it, what it predicts, & the evidence-based interventions that work

It sounds funny at first…until it’s not.
Morning wood is one of the most reliable gauges of integrative health function across five systems: vascular, metabolic, hormonal, circadian, & nervous.
Yet one component that gets left out of most PCP conversations is this: the loss of these events over time often precedes diagnosable cardiovascular disease cases 5-10 years in advance.
We’re trained to believe it’s purely about libido, but there’s way more to it. The complexity behind morning wood is exactly what makes it such an elite leading indicator for future health outcomes.
Here’s what your morning wood (or lack thereof) is telling you.

The Biological Drivers
Search for “morning wood” in academic research and you’ll come up empty. The formal term is nocturnal penile tumescence (NPT) — defined as spontaneous erections occurring during REM sleep.
Unlike erotically induced erections that are psychogenic, morning wood is purely physiological. It’s driven by the parasympathetic nervous system and the release of nitric oxide from the endothelium and nitrergic nerves.
During REM sleep, your brain downregulates sympathetic tone & upregulates parasympathetic activity1. This shift triggers a series of events across multiple systems in the body enabling increased blood flow to the penis.
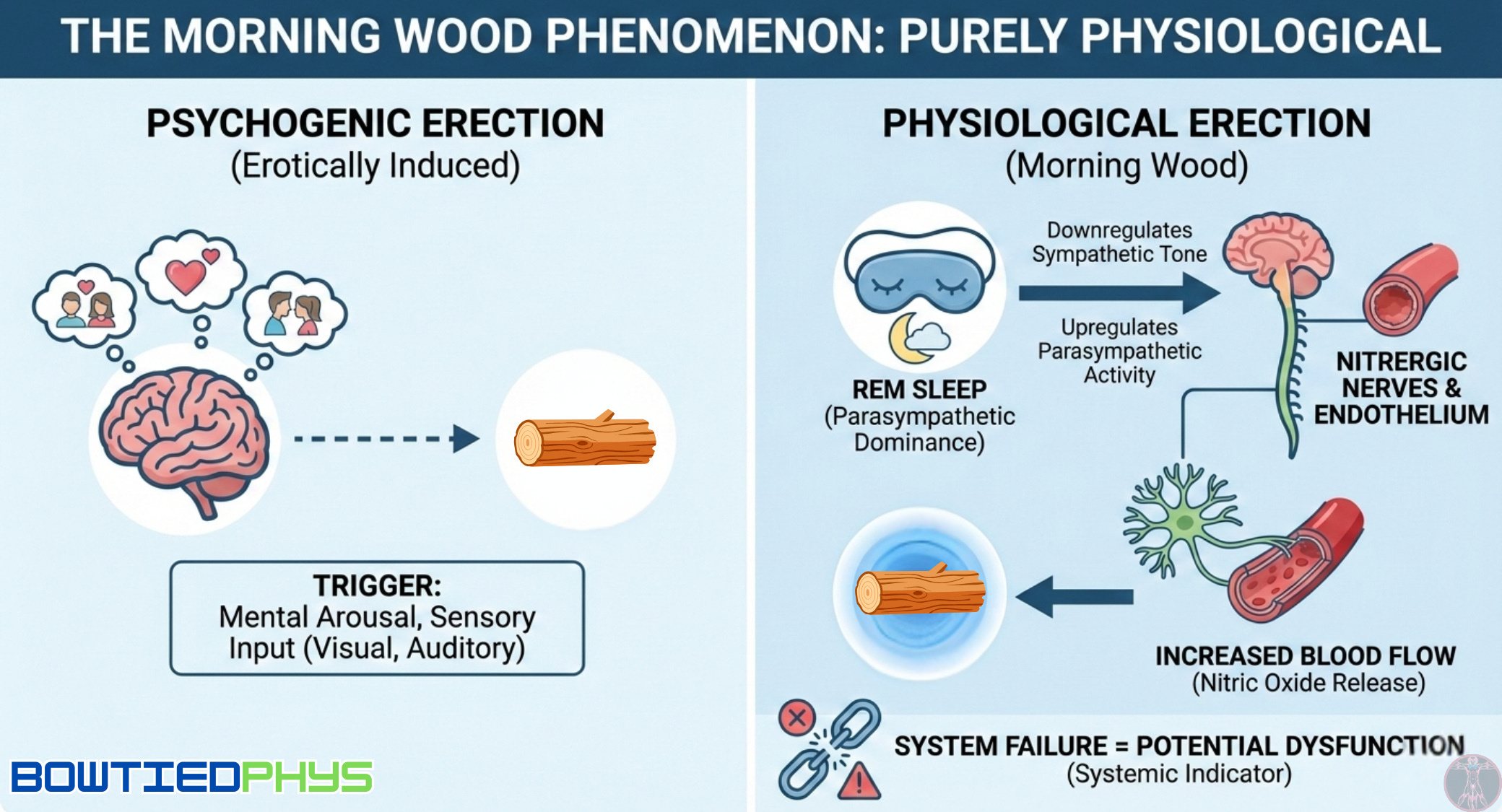
When this highly integrated system fails, it reveals a dysfunction somewhere in the chain.
The Five Systems Test
Morning wood’s clinical power lies in its dependence on multiple systems working in cooperation. Its presence confirms functional integrity. Its absence signals compromise across one or more pathways.
System 1 → Endocrine System: Androgens
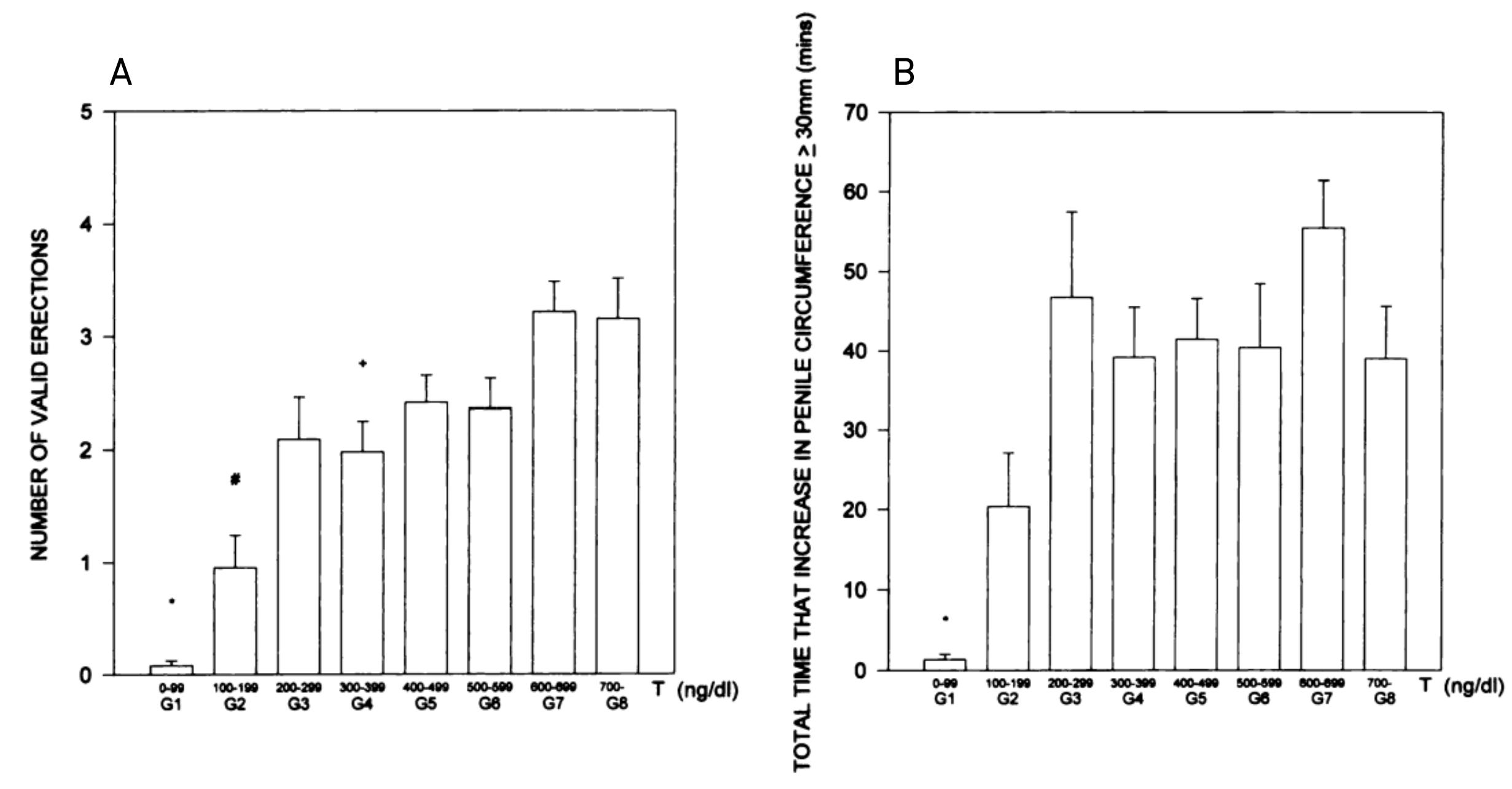
Testosterone is the main hormonal regulator of morning wood and the relationship is dose-dependent. Granata et al. (1997)2 studied 201 men and found that below 200 ng/dL serum testosterone, morning wood becomes suboptimal or disappears entirely.
But testosterone doesnt working alone. Dihydrotestosterone (DHT), the 5α-reduced metabolite of testosterone, plays an equally critical role. When 150 men aged 50–70 years3 received transdermal DHT treatment, early-morning erections improved significantly after three months.
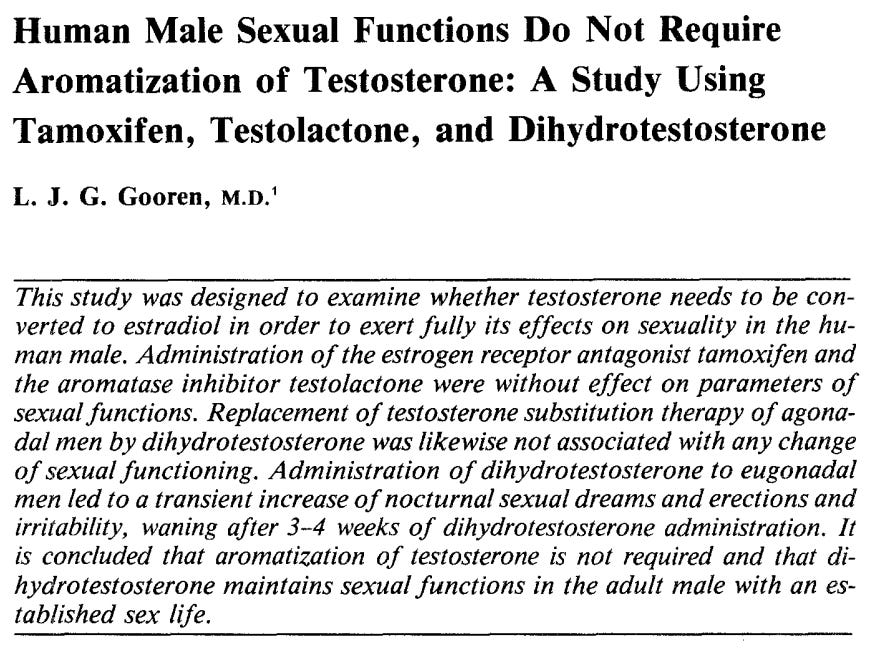
Gooren at. (1985)4 showed DHT therapy not only improved morning wood but increased nocturnal sexual dreams.
Foresta et al. (2003)5 similarly demonstrated that transdermal DHT therapy significantly improved morning wood in hypogonadal men and that DHT acts as the active androgen in maintaining nitric oxide-mediated erectile activity.
System 2 → Neurohormonal System: Dopaminergic Pathways
Initiating and maintaining morning wood depends on central dopaminergic signaling.
Testosterone increases nitric oxide synthase (NOS) activity in the medial preoptic area of the brain — a region critical for sexual behavior. The flow works like this: testosterone pulse → activation of central NOS → increased peripheral NO → dopamine release → morning wood.
Interestingly, dopamine’s role here differs from its role in waking erections. Dopamine uptake inhibitors improve stimulus-bound erections during wakefulness6 but paradoxically reduce morning wood & REM sleep.
System 3 → Circadian & Sleep Architecture
Morning wood is coupled with REM sleep architecture. The sleep-related rise in serum testosterone7 is linked to the appearance of the first REM episode establishing a bidirectional relationship: sleep architecture influences testosterone secretion AND testosterone modulates sleep quality.
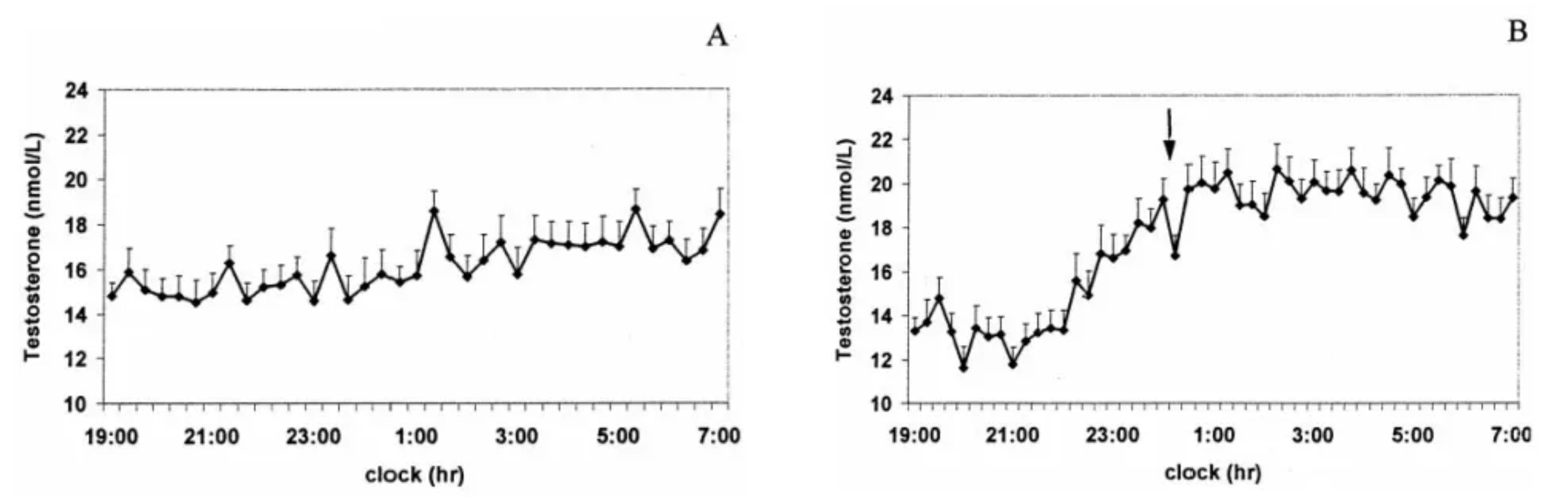
Schiavi et al. (1992)8 also found age-independent positive associations between sleep efficiency, decreased REM latency, number of REM episodes, and circulating testosterone levels.
System 4 → Nervous System Regulation: Parasympathetic Tone
Morning wood generation is a parasympathetic event. The penile erection reflex9 operates through sacral parasympathetic nerve fibers (S2-S4), which release acetylcholine and activate nitrergic nerve endings in the penis.
Without taking your foot off the sympathetic gas, the parasympathetic brake will never be engaged (morning wood becomes implausible).

System 5 → Endothelial Function: Blood Flow & NO Bioavailability
The most consequential system interrogated by morning wood.
Nitric oxide (NO) produced by endothelial nitric oxide synthase (eNOS) acts as the molecular signal for systemic vascular vasodilation. When NO bioavailability is compromised, the morning erection potential suffers.
Because penile arteries are smaller in diameter10 (1–2 mm) than coronary arteries (3–4 mm), the same degree of endothelial dysfunction produces disproportionately greater reduction in penile blood flow.

The penis is a more sensitive barometer of systemic endothelial health than the heart itself. This is precisely what makes it predictive for cardiovascular disease.
The Cardiovascular Connection
So how is not having morning wood the canary in the CVD coal mine?
The relationship between morning wood & CVD is more than correlational given its mechanistic roots in shared vascular biology. And the epidemiological evidence grows stronger every few years.
Here are some of the data:
ED is present in > 50% of men with a history of CVD11.
1 in 8 men with ED12 reports a prior cardiovascular event.
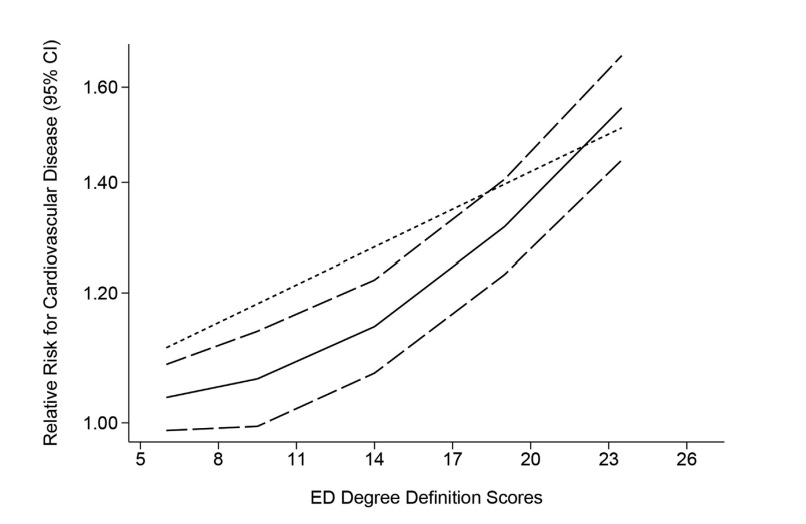
A meta-analysis across 154k men with ED13 showed relative risk increases of 59% & 34% for ischemic heart disease & stroke, respectively.
The greater the ED severity = the greater the CVD risk.
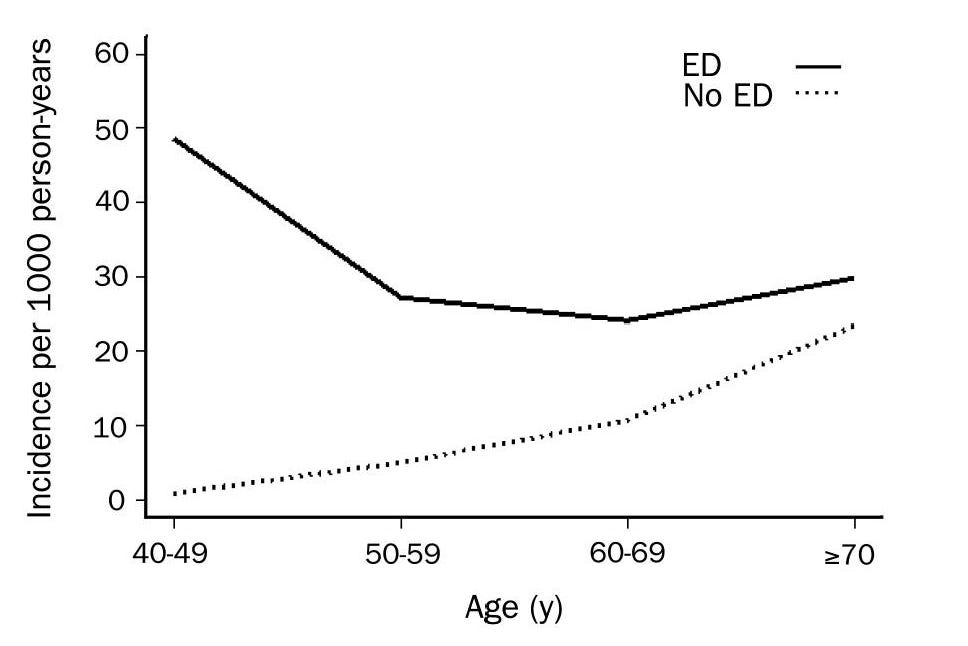
The ED signal becomes even more powerful in younger men. Among men aged 40–49 years, the incidence of heart disease in those with ED was nearly 50 TIMES higher14 than in men without it.
In 1991, Gossetti et al.15 evaluated sexual function in men with advanced atherosclerosis. Of 386 patients, 148 (38%) reported prior erectile dysfunction. When 44 underwent preoperative testing, all 44 showed impaired morning wood: 77% had complete absence, 23% had mild absence.
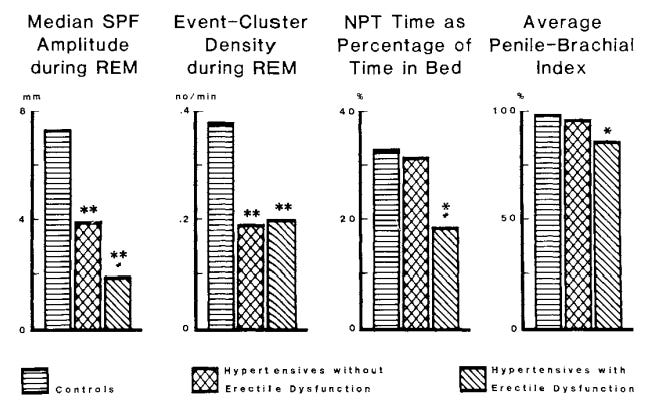
Penile blood flow studies conducted by Karacan et al. (1989)16 demonstrated a stepwise reduction in penile blood flow amplitude across three groups. Morning wood degradation represents a continuum of vascular compromise that tracks with systemic arterial disease.
Not Just for Men
Women experience the same phenomenon — nocturnal clitoral tumescence, or what we’ll call “morning bean.”
During REM, parasympathetic-mediated increases in pelvic blood flow produce clitoral engorgement and vaginal lubrication in women17. The same endothelial dysfunction, parasympathetic neuropathy, & NO signaling deficits that degrade morning wood in men also impair sleep-related blood flow in women.
Female sexual dysfunction shares overlapping vascular/neurological risk factors with male ED: hypertension, diabetes, & metabolic disease. Therefore, the biological rationale for treating a lack of morning wood/bean as a systemic health indicator is equally sound for both sexes.
The Functional & Integrative Solution Stack
Now that you understand why morning wood is one of the most critical measures of vitality, here’s how to improve your own Morning Wood System.
Circadian Biology & Sleep Architecture
Daily sunlight → Minimum effective dose = 10 min ~sunrise + 10 min ~sunset + 30 min around peak UV hours. Red/NIR exposure on thyroid/pelvic areas for fertility & parasympathetic support.
Consistent wake/bed times → Embrace 24-hr rhythmicity. Test Epitalon to regulate the clock.
Light environment at home → Minimal overhead lights at night. Replace LEDs with incandescents. Blue light blockers/Night Shift Mode. Add vitamin D lamp if seasonal affective disorder is present.
Optimize sleep conditions → Total blackout in bedroom. 60–64 °F. Hot shower before bed. Nasal breathe w/ mouth tape (SomniFix or 3M micropore).
Kill nnEMF sources at night → WiFi routers. Bluetooth. Phones.
Supplement strategically before bed → 400—600 mg magnesium + 3—5g glycine + 400—600 mg L-theanine + 1—2g myo-inositol.
Nervous System Regulation
Analog brain dumps before bed → An effective anti-anxiety tool.
24-hour social media fast → 1x weekly. Regular digital detachment preserves attention span & mental clarity.
Curate your digital signal-to-noise ratio → Mute words aggressively. Delete sources of chronic doomerism. Ignore > negatively engaging.
Embrace life as a two-player game → It’s today you versus last week you. It doesn’t get easier, but it gets simpler.
Metabolic Health
Resistance training → 3—4x/week
Fasted low-intensity cardio → 30—45 min sessions 3-4x/week (avoid excessive Z3+ training > 250 min/week)
HIIT → 1—2 sessions/week (HR should be above 90% max)
Post-prandial walks → Walk post meals 10—15 min. Stand for 45 min if unable to walk.
Keep body fat < 18% → Ideally 12—15% as a male.
Use daylight diet/time-restricted feeding → Big breakfast. Medium lunch. Small dinner > 2 hrs before bed.
Test metabolic biomarkers → Guide provided below with functional ranges.

Oral Microbiome
Switch to nano-hydroxyapatite toothpaste → Remineralizes enamel without the negative impacts of fluoride-based products.
Scrape your tongue daily → Removes bacteria that brushing misses & improves oral microbiome health.
Avoid alcohol-based mouthwash → Destroys beneficial oral bacteria, dries protective mucosa, & negatively impacts vascular function.
Functional Nutrition
Embrace functional foods & herbs → Pasture-raised eggs. Raw local honey. Watermelon. Pomegranate. Oysters. Cacao. Wild-caught salmon. Ginger. Saffron.
Critical micronutrients → Balance Zn:Cu ratio (~10:1). All B vitamins. Vitamins A, C, E, K2 (via whole foods). Magnesium (1g elemental/day). Selenium (2—3 Brazil nuts/day). Vitamin D (via sunlight). Iodine. Molybdenum.
Take care of the gut → Consume fermented foods (kimchi, kefir, sauerkraut, yogurt), bone broth/collagen, & prebiotics (green bananas, gluten-free oats, garlic, apples, onions). Cycle glutamine or BPC-157 if needed.
Supplementation → Nattokinase. Taurine. Ginkgo biloba. Alpha-GPC. Ubiquinol. L-citrulline. PT-141 (nuclear option once foundations locked in).
As with every bioindividualized protocol you develop — apply tactics that only fit the strategy & prioritize subtractions/substitutions before additions.
That’s all for this week. DMs & comments are open for any questions/more specifics.
See you guys next week.
Your friend,
Phys
Giuliano F, Rampin O. Neural control of erection. Physiol Behav. 2004 Nov 15;83(2):189-201. doi: 10.1016/j.physbeh.2004.08.014. PMID: 15488539.
Granata AR, Rochira V, Lerchl A, Marrama P, Carani C. Relationship between sleep-related erections and testosterone levels in men. J Androl. 1997 Sep-Oct;18(5):522-7. PMID: 9349750.
Kunelius P, Lukkarinen O, Hannuksela ML, Itkonen O, Tapanainen JS. The effects of transdermal dihydrotestosterone in the aging male: a prospective, randomized, double blind study. J Clin Endocrinol Metab. 2002 Apr;87(4):1467-72. doi: 10.1210/jcem.87.4.8138. PMID: 11932266.
Gooren LJ. Human male sexual functions do not require aromatization of testosterone: a study using tamoxifen, testolactone, and dihydrotestosterone. Arch Sex Behav. 1985 Dec;14(6):539-48. doi: 10.1007/BF01541754. PMID: 4084053.
Foresta C, Caretta N, Garolla A, Rossato M. Erectile function in elderly: role of androgens. J Endocrinol Invest. 2003;26(3 Suppl):77-81. PMID: 12834027.
Andersen ML, Tufik S. Inhibitory effect of GABAergic drugs in cocaine-induced genital reflexes in paradoxical sleep-deprived male rats. Pharmacol Biochem Behav. 2004 Jun;78(2):301-7. doi: 10.1016/j.pbb.2004.04.003. PMID: 15219771.
Luboshitzky R, Zabari Z, Shen-Orr Z, Herer P, Lavie P. Disruption of the nocturnal testosterone rhythm by sleep fragmentation in normal men. J Clin Endocrinol Metab. 2001 Mar;86(3):1134-9. doi: 10.1210/jcem.86.3.7296. PMID: 11238497.
Schiavi RC, White D, Mandeli J. Pituitary-gonadal function during sleep in healthy aging men. Psychoneuroendocrinology. 1992 Nov;17(6):599-609. doi: 10.1016/0306-4530(92)90018-3. PMID: 1287680.
Dean RC, Lue TF. Physiology of penile erection and pathophysiology of erectile dysfunction. Urol Clin North Am. 2005 Nov;32(4):379-95, v. doi: 10.1016/j.ucl.2005.08.007. PMID: 16291031; PMCID: PMC1351051.
Yannas D, Frizza F, Vignozzi L, Corona G, Maggi M, Rastrelli G. Erectile Dysfunction Is a Hallmark of Cardiovascular Disease: Unavoidable Matter of Fact or Opportunity to Improve Men's Health? J Clin Med. 2021 May 20;10(10):2221. doi: 10.3390/jcm10102221. PMID: 34065601; PMCID: PMC8161068.
Montorsi F, Briganti A, Salonia A, Rigatti P, Margonato A, Macchi A, Galli S, Ravagnani PM, Montorsi P. Erectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery disease. Eur Urol. 2003 Sep;44(3):360-4; discussion 364-5. doi: 10.1016/s0302-2838(03)00305-1. PMID: 12932937.
Corona G, Rastrelli G, Maseroli E, Fralassi N, Sforza A, Forti G, Mannucci E, Maggi M. Low testosterone syndrome protects subjects with high cardiovascular risk burden from major adverse cardiovascular events. Andrology. 2014 Sep;2(5):741-7. doi: 10.1111/j.2047-2927.2014.00241.x. Epub 2014 Jul 7. PMID: 25044637.
Zhao B, Hong Z, Wei Y, Yu D, Xu J, Zhang W. Erectile Dysfunction Predicts Cardiovascular Events as an Independent Risk Factor: A Systematic Review and Meta-Analysis. J Sex Med. 2019 Jul;16(7):1005-1017. doi: 10.1016/j.jsxm.2019.04.004. Epub 2019 May 16. PMID: 31104857.
Inman BA, Sauver JL, Jacobson DJ, McGree ME, Nehra A, Lieber MM, Roger VL, Jacobsen SJ. A population-based, longitudinal study of erectile dysfunction and future coronary artery disease. Mayo Clin Proc. 2009 Feb;84(2):108-13. doi: 10.4065/84.2.108. PMID: 19181643; PMCID: PMC2664580.
Gossetti B, Gattuso R, Irace L, Intrieri F, Venosi S, Benedetti-Valentini F. Aorto-iliac/femoral reconstructions in patients with vasculogenic impotence. Eur J Vasc Surg. 1991 Aug;5(4):425-8. doi: 10.1016/s0950-821x(05)80175-6. PMID: 1915908.
Karacan I, Salis PJ, Hirshkowitz M, Borreson RE, Narter E, Williams RL. Erectile dysfunction in hypertensive men: sleep-related erections, penile blood flow and musculovascular events. J Urol. 1989 Jul;142(1):56-61. doi: 10.1016/s0022-5347(17)38661-5. PMID: 2733110.
Woodard TL, Diamond MP. Physiologic measures of sexual function in women: a review. Fertil Steril. 2009 Jul;92(1):19-34. doi: 10.1016/j.fertnstert.2008.04.041. Epub 2008 Nov 30. PMID: 19046582; PMCID: PMC2771367.
“Morning bean” took me out
The smaller-caliber point is what makes this click. Penile arteries at 1 to 2 mm versus coronaries at 3 to 4 mm means the same endothelial dysfunction shows up in the penile circulation years before it registers at the heart. That turns NPT loss from a libido footnote into an early vascular readout.
The nearly 50x heart disease incidence in the 40 to 49 ED group is the stat that should end the "just stress" conversation.
When a younger man reports losing morning erections but has a clean lipid panel, where do you look first, endothelial function or the androgen side?