

Reclaim Your Potency
Drive and sexual function are collapsing in men under 35. The 15 upstream fixes to get yours back (and then some).

If your great-grandfather were alive today, he’d be horrified at the thought of his 25 yr-old self being plagued by a disease of the elderly.
Now we’re in the midst of a silent epidemic.
It’s the single most common issue men in their 20s and 30s ask me about — they can’t get it up. Or they can, but their drive sucks. Morning wood vanishes. Vitality lost. Sex embarrassingly bad.
It’s the same story over & over again:
Can’t get it up.
Take the PDE5 inhibitor (tadalafil or sildenafil).
All is well.
Come off.
Limp again.
Just anecdotal?
Nope.
More than HALF of all guys under 35 are experiencing erectile dysfunction, while 75% suffer in silence.

One pediatric urology practice just found a 31x increase in teenage males with ED since 2014.
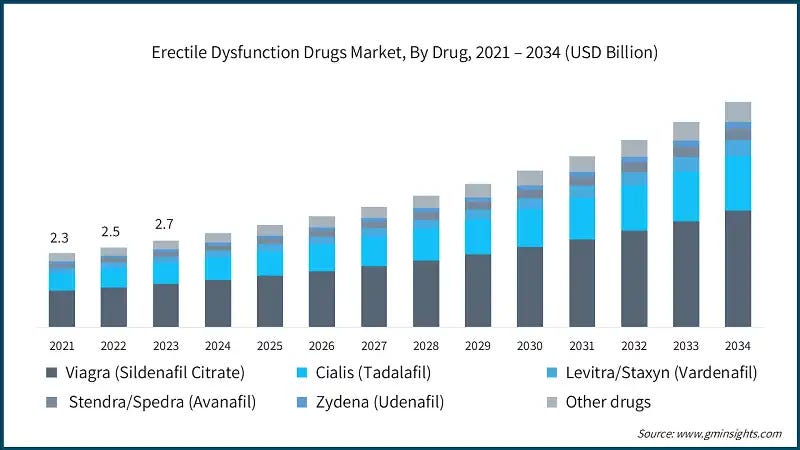
Still not buying it? Then follow the money and it’ll make more sense: the ED drug market already clears $3 billion a year and is projected to double by 2033.
Here’s the good news: ~90% of cases are reversible when you address the root causes early enough. And the sooner you address them, the better. Upstream damage that’s easy to reverse at 25 becomes a decade of dysfunction by 35.
But we’ve been having the wrong conversation.
For the past decade, the health space has offered a single villain: “It’s the porn!” It’s repeated ad nauseam and nothing has changed (situation has only worsened).
The explanation isn’t wrong. It’s just reductionist, incomplete, and frankly lazy. We build strategies here. We don’t hunt tactics.
So it’s time to go upstream. To the 5 systems & 15 causal factors actually driving the modern flaccidity epidemic.
System 1: Vascular Engine
Factor #1 — Cardiometabolic dysfunction
How
Body fat past ~20% kills erection quality: Excess visceral fat is a cocktail of aromatase + poor mitochondrial function + inflammation + leptin/insulin resistance.
Combined high-fat & high-carb breaks metabolic flexibility: Hyperpalatable foods (highly processed) impairs glucose oxidation. Clean carb oxidation generates the CO₂ driving vasodilation & libido.
Metabolic slowdown makes a low-energy state: Low thyroid. Low gut short-chained fatty acids (SCFAs). Elevated chronic stress hormones. Micronutrient scarcity.
ED² (Endothelial Dysfunction = Erectile Dysfunction): Leptin/insulin resistance, low-grade chronic inflammation, & oxidative stress suppress NO signaling in the tiny helicine arteries of the penis well before the coronaries. It’s why ED is the earliest canary in the CVD coal mine.
Evidence
A 2025 analysis found metabolic disease raised ED odds 2.3x.
Molina-Vega et al. (2019) reported 42% ED prevalence in non-diabetic obese men.

In 193 young men with early coronary disease, ED prevalence was 57.8% vs. 31.1% in controls.
Fix
Track cardiometabolic health biomarkers: See below.

Build your aerobic engine (most validated non-drug ED fix): A 2023 RCT meta-analysis improved erectile function 2.3–4.9 points. Base building with 60+ min daily of low-level aerobic movement (walks) & 2–4 focused sessions (1–2 HIIT & 1–2 moderate intensity).
Build muscle as a glucose sink: Lift 3–4x/week. Clears glucose & improves androgen signaling.
Fix fuel partitioning: Favor clean carbs (potatoes + rice + fruit) without added fats. Avoid high-fat + high-carb combos that drive insulin resistance. Warm hands/feet, no post-meal crashes, & morning wood are solid biofeedback forms.
Drop to ~12–15% body fat: Strips the aromatase converting your testosterone to estrogen.
Support the mitochondrial cofactors/substrates: B-vitamins. Creatine. Magnesium. Ubiquinol (preferred CoQ10 source). Taurine. PQQ. K2. Zinc/copper (balanced to ~10:1).
Hold off on TRT: Lose the visceral fat first. Then weigh the decision. A 2014 RCT found it didn’t fix insulin resistance or visceral adiposity.
Factor #2 — Redox imbalance
How
Modern stress bottlenecks the electron transport chain: Concentrated blue light. nnEMF. High Omega-6/Omega-3 loads. Mouth breathing. Endotoxin. Nutrient gaps. Electrons leak → reactive oxygen species spike → depletes glutathione (master antioxidant) → NADH backs up (reductive stress) → lactate increases.
Stressed mitochondria deprioritize sex steroids: Cholesterol reroutes toward cortisol in what is known as the pregnenolone steal & androgen receptors get sequestered. Total T levels usually will read as normal (deceptively).
Imbalanced GABA/glutamate drives excitation: Glutamate & Ca²⁺ influx (cortisol, adrenaline, blue light, nnEMF) collapse mitochondrial membrane potential and spike ROS.
Low T3 starves the system: Weak thyroid impairs mitochondrial biogenesis & ATP production further tanking steroidogenesis & Leydig responsiveness to LH.

Evidence
Xu et al. (2024) found that better oxidative balance scores built from 16 dietary and 4 lifestyle components tracked with lower ED risk.
Fix
Rebuild ETC cofactors: Thiamine (B1). All B-vitamins (B2/B3/B5/P5P/B9/B12). Ubiquinol. Taurine. Magnesium. Balanced copper/zinc & selenium/iodine. Adequate saturated fat.
Load testicular antioxidants to protect sperm from peroxidation: NAC. Taurine. Tyrosine. Vitamin E + C. Ubiquinol. L-carnitine. Selenium. Ginger. Creatine. to protect Leydig cells and .
Eliminate oxidative inputs: Seed-oil PUFA. Alcohol. Hyperpalatable processed foods.
Support glucose oxidation & thyroid: Carbs timed with light (breakfast w/ sunrise & lunch w/ UV-B midday sun). Avoid high Omega-6 & estrogenic toxins. Supplement T3 if needed.
Deploy targeted libido tools: Low-dose tadalafil (5 mg). Tribulus. Black ginger. Capsaicin-based foods. Agmatine sulfate. Red/IR on the balls. Brief cold exposure.
Clear the upstream stressors first: Fix gut/endotoxin (#4). Lower prolactin/serotonin excess. Balance pregnenolone/progesterone (#11).
Factor #3 — Micronutrient depletion
How
Sad story of SAD: Standard American Diet is one of micronutrient insufficiency (undernourished) & caloric excess (overfed).
Modern depletion outpaces intake: Soil depletion. Processed/plant-heavy diets. Hydrogenated vegetable oils. Gut dysbiosis. All cut absorption and raise demand for the cofactors Leydig cells need for cholesterol side-chain cleavage and steroidogenesis (zinc, copper, magnesium, retinol, B-vitamins, selenium, electrolytes).
Zinc depletes first: The cofactor for testosterone synthesis, LH signaling, and aromatase control. Drains from tissues for years before labs reflect. Then low T, high estrogen, wrecked sperm count/motility/morphology, weak libido.
Copper collapses on unbalanced zinc: Cytochrome c oxidase loses efficiency, dopamine synthesis falls (tyrosine hydroxylase), thyroid conversion stalls, and iron gets trapped. All starve gonadal energy & NO production.
Magnesium burns under high stress, excess blue light, & nnEMF: SHBG rises (locking up free T), vascular smooth muscle can’t relax, and mitochondrial ATP decreases.
Fat-soluble vitamins fail without synergy: Retinol, E, K2, & D need dietary fat and ratio balance.
Gut damage compounds it: Endotoxin & low-grade inflammation block nutrient transporters and raise burn rate. So even adequate intake is inadequate that never reaches the gonads.
Use caution with a diversity-lacking gym-bro diet: Chicken/rice/veg without organ meat means no heme iron, poor zinc:copper ratio, no choline. All meaning it’s easier for mitochondrial failure & dopamine to crash.
Evidence
Men on a micronutrient-dense Mediterranean diet show significantly lower ED risk.

Liao et al. (2024) found unexpectedly high ED rates in GLP-1 users → micronutrient depletion during rapid weight loss.
Fix
Test then address (deficiencies): Confirm gaps where you can (RBC magnesium, serum zinc/copper, ferritin/serum iron/TIBC/saturation, plasma homocysteine, serum 25(OH)D, serum B9/B12). Track intake closely for 8–12 weeks. Then maintain.
Fix the gut first for enhanced absorption (#4): Or you’re just pouring high-quality foods & supplements down the inflamed/leaky gut drain.
Integrate the ancestral micronutrient stack: Oysters (zinc/copper/selenium/B12). Dark/organ meats (retinol, copper, folate). Egg yolks (choline, K2). Red meat (zinc, heme iron, carnitine). Full-fat dairy (calcium, magnesium, iodine).
Balance the antagonists: Never megadose zinc without copper. Pair magnesium with a 2:1 potassium to sodium ratio. Keep retinol and D in ratio with E and K2.
Replenish electrolytes aggressively: Magnesium (taurinate/pidolate /glycinate/chloride/sucrosomial). Potassium (coconut water/potatoes). Sodium. All critical for CO₂ tolerance & vascular relaxation.
Cover the missed mitochondrial cofactors: B2/B3/B5/P5P/B9/B12, manganese, taurine, glycine, tyrosine to keep the ETC running.
Add the NO-pathway lever: L-citrulline 6–8g/day (superior bioavailability to L-arginine which saw a 74% improvement in vasculogenic ED)
Factor #4 — Leaky gut & microbiota dysbiosis
How
Modern environments spike zonulin & shred tight junctions: Isolated blue light. nnEMF. High Omega-6/low Omega-3 intake. High pesticide exposure. Low stomach acid. Excessive intense exercise without recovery. Poor circadian consistency. Endotoxin flood in → trigger systemic & neuroinflammation → blocks androgen & progesterone receptors.
Low stomach acid lets the upper GI overgrow: Fermentation & pathogens grow leading to an imbalance of the “good” bacteria to “bad” bacteria ratio. Malabsorption of the zinc, copper, B-vitamins, & magnesium that testosterone synthesis depends on occurs.
Training without fuel & fiber accelerates gut leak: Exercise drops gut blood flow. Missing soluble fiber (from fruit) gives a gut barrier breaking down faster than it rebuilds tanking thyroid conversion & NO bioavailability.
Dysbiosis nukes the gut lining: Lost butyrate & SCFAs deteriorate gut lining enterocyte mitochondria → thin the mucus layer → leaky gut/more porous → amplify cytokines & reactive oxygen species → dysregulate vagus nerve & HPA axis.

Evidence
Schmidt et al. (2019) found 94% of inflammatory bowel disease patients reported ED symptoms. Geng et al. (2021) reported lower microbiome diversity in ED patients.

Fix
Heal the gut with the 6R framework.
Recon: Assess before you intervene
Track at-home signals daily: Morning wood frequency and strength. Pre-caffeine AM blood pressure. Energy-to-anxiety ratio (spread across day). Digestion. Facial puffiness. Skin clarity. Headaches. Stool frequency & Bristol type. Breath.
Order a comprehensive stool panel (like Genova or Doctor’s Data): Dysbiosis. Pathogens. Calprotectin. Zonulin. Pair with an organic acids test (OAT) for fungal and bacterial metabolites.
Pull the systemic inflammation markers: hs-CRP. Homocysteine. Metabolic biomarkers.
Run the gut-critical nutrient panel: RBC magnesium. Serum zinc & copper. Ferritin/serum iron/TIBC/saturation. 25(OH)D. Serum B9/B12 (w/ MMA if borderline).
Map the gut-adjacent hormones: Total & free testosterone. SHBG. E2 (sensitive assay estradiol). Prolactin. LH/FSH. TSH. Free T3 & T4.
Remove: Strip the triggers
Strip dietary triggers: Seed-oil PUFA. Gluten. Ultra-processed hyperpalatable combos (high-fat + high-carb + MSG + additives). Industrial dairy, soy, alcohol, & high-FODMAP foods.
Cut food-additive barrier disruptors: Carrageenan. Polysorbate-80. Food dyes. Artificial sweeteners. All directly damage tight junctions.
Eliminate Big Pharma and toxin loads: NSAIDs & PPIs. Glyphosate (choose organic). Fluoride (filter your water). Address environmental mold exposure.
Calm the nervous system input (cross-ref #11, #12, #15): GABAergic compounds. Resting heart rate reduction/breathwork. Digital fast. Brain dumps. Analog systems. Time outdoors in green.
Reduce: Lower the systemic inflammation
Bind endotoxin and metals: Modified citrus pectin 5–8g in between meals.
Disrupt biofilm presence: Nattokinase 10,800 FU/day. NAC 600–1,200mg/day. Lactoferrin 250–500mg/day.
Supply the repair raw materials: Bone broth 1–2 cups/day as food-first lever OR glycine 3–5g + collagen 10–20g/day to feed the mucus matrix & connective tissue
Run targeted anti-inflammatory herbs: Black seed oil (Nigella sativa) 2–4g/day. Ginger 2–4g/day. Organic, heavy metal tested cinnamon 3–5g/day. Oregano oil 50–100 mg/day.
Deploy the advanced peptide stack (every other day): BPC-157 250–500mcg/day (oral). KPV 500mcg–1mg/day.

10% off w/ PHYS10 @ checkout
Repair: Rebuild the barrier
Restore stomach acid and motility before any lining-repair work: Sea salt (Diamond Crystal Iodized Salt or Jacobsen) & adequate sodium to supply chloride for HCl. Thiamine (B1) 100–200mg/day for gastric motility & vagal tone. Bitter herbs pre-meal (chamomile, gentian, dandelion, ginger) to trigger HCl and bile. Chew thoroughly and stop snacking so the migrating motor complex can clear the upper GI between meals. Test for and treat H. pylori if suspecting.
Rebuild tight junctions and mucus: L-glutamine 20–30g/day (primary enterocyte fuel). Zinc-carnosine 75mg twice daily.
Feed enterocytes directly: Tributyrin 500–1,500mg/day for SCFAs delivery direct to the gut lining with less dependence on a working microbiome.
Titrate fiber: Top 3 sources (partially hydrolyzed guar gum (PHGG), acacia fiber, psyllium husk). Start @ 1g & add 1 g/week working up to 3g/day. Stop if poor digestion or cramps.
Reinoculate: Repopulate after the barrier is sealed
Clear biofilms: Nattokinase 10,800 FU/day. NAC 1,200mg/day. Lactoferrin 250–500mg
Run a pulsed antimicrobial for 2–4 weeks: Berberine 500–600mg, 2–3x/day. Oregano oil 50–100mg/day. Black seed oil 1–2g/day. Rotate between agents to avoid resistance.
Reseed with food-first targeted probiotics: Saccharomyces boulardii (kefir, kombucha, kvass, miso). L. reuteri (kefir, sauerkraut, kimchi, yogurt). Spore-based Bacillus subtilis (natto, miso). Akkermansia muciniphila (pomegranate arils/juice/whole, blueberries, walnuts)
Layer prebiotics once the lining is sealed: PHGG 5–10g/day or acacia fiber 5–10g/day to feed new flora.
Reload the gut-healing micronutrients (full stack in #3): B vitamins. Zinc/copper. Retinol. Magnesium. Wild-caught fish. Grass-fed meats.
Rebalance: Dial in the maintenance phase
Eat in a screenless parasympathetic state: Chew thoroughly. No eating while stressed or scrolling (cross-ref #12).
Anchor meal timing to the clock: Eat a daylight diet on a consistent day-to-day schedule. Finish 3+ hours before bed (cross-ref #13, #15).
Move after meals: 10–15 minutes to improve digestion, glycemic response, & bile flow.
Treat sleep & stress as gut interventions: Poor sleep raises zonulin and endotoxemia within days (cross-ref #11, #13, #14).
Protect the gut on training days: L-glutamine 10–20g + 20g collagen around intense or fasted/endurance work.
Maintain the microbiome with food (full stack in #3): Organic. Mineral-dense. Fermented foods (yogurt, kefir, kimchi, miso, natto).
Eat the occasional raw carrot salad between meals: One medium raw carrot dressed with a pinch of sea salt + a teaspoon of EVOO, & a splash of vinegar. The insoluble fiber binds bacterial endotoxin & excess estrogen out of the gut before they can be reabsorbed.
Rerun Phase 1 Recon quarterly: Continue tracking at home signals daily & metabolic/inflammatory markers every 6 months

Factor #5 — Nicotine
How
Vasoconstrictor & a vascular toxin: Nicotine spikes sympathetic tone & constricts arteries acutely. Chronic use drives oxidative endothelial damage & kills NO bioavailability.
Sympathetically pinned: Chronic nicotine elevates adrenaline/cortisol tone — the opposite of the parasympathetic state an erection requires (Factor #12).
“Focus/dopamine” defense is a trap: Yes, nicotine bumps dopamine and acetylcholine acutely…but that’s exactly how it builds a habit loop downregulating baseline drive & speedrunning an anhedonic natural state.
Evidence
A double-blind, placebo-controlled RCT by Harte & Meston (2007) showed nicotine cut erectile response by 23%.

El-Shahawy et al. (2022) found e-cigarette users over twice as likely to report ED.
Fix
No dose will ever help your erectile quality.
Here’s exactly how to take the offramp:
Nicotine Exit Protocol

You’ve been psy-op’d into believing you can spam Zyns without biological consequence. But wanting to quit and building the proper exit are two different things.
Factor #6 — Weed
How
THC suppresses the HPG axis: CB1 activation in the hypothalamus blunts GnRH pulses → lower LH/FSH → lower testosterone + higher prolactin (elevated prolactin alone tanks libido & erectile quality)
Chronic use disrupts NO peripherally: Acute low-dose cannabinoids transiently vasodilate, but spamming too impairs endothelial NO signaling.
The wrong blunt…of dopaminergic drive: Downregulated motivation/arousal circuitry compounds the hormonal hit.
Evidence
Pizzol et al. (2019) found that daily users had 2.7x higher ED odds than non-users.
Fix
Taper to zero: Lower frequency. Take an extended break. Then reassess.
Lower prolactin actively: B6 (P5P), zinc/copper (~12:1 ratio), selenium/iodine (~1:1 ratio) and tyrosine (1–2g on empty stomach in AM). Check prolactin on labs if libido stays low after quitting.
