

The Case for Broscience
How the Broscientist Became the Health Space's Sovereign Individual

Last week, Balaji Srinivasan — the mastermind behind The Network State —doubled down on a prediction he made a couple years ago:
He was referencing his 2023 statement on self-experimentation as the basis for distributed research:

He’s right. And we’re watching it happen in real-time.
Once dismissed as gym bro pseudoscience (still is by many), broscience is evolving into the dominant framework for advancing health outcomes. Not because it’s replacing academic science, but because it’s filling the gaps academic research can’t reach: individual variability, long-term outcomes, & optimization at the margins of human performance.
It’s not strictly about bodybuilding anymore. It’s about the decentralization of medical knowledge, the democratization of diagnostic tools, & the rise of the sovereign individual in health.
Now feels like the opportune time to examine what the future of health & fitness holds — and why that future is broscience.
What Even Is Broscience & Why Should We Care?
Broscience is the ultimate success story of valuing independent replication over prestigious citation. It’s the rawest, most practical application of scientific inquiry. It’s rooted in real-world outcomes and requires a hypersensitivity to biofeedback. It’s the ultimate “skin in the game”. It’s self-experimentation in its purest form — leading to the observation of cause-and-effect and eventual discernment of applied principles for training, healing, & optimizing the body. It’s the act of blending historical practices with interdisciplinary critical thinking & experimental anecdotes taking the n = 1 → 10 → 10,000.
In the context of history, the principles undergirding broscience are nothing new. Before the rise of centralized health research institutions, advancing understanding through direct observation was the norm — not a violation of scientific method, but an embodiment of the method.
Early Chinese observed more organ malfunctions1 (cardiovascular disease, diabetes) in physically inactive populations.
Greek physician Galen2 (175 AD) prescribed “vigorous motion” to purge toxins.

In 600 BC, Indian physician Sushruta3 recommended moderate physical activity to balance the three doshas (vata, pitta, & kapha) and observed that sedentary lifestyles led to kapha accumulation.
Today, this approach is having its moment in the health spotlight. Another symptom of “history running in reverse”. What started as gym experimentation culture decades ago is evolving into a comprehensive health optimization methodology.
Why The Broscientist Is The New Sovereign Individual
Technology reduced the power of centralized nation-states. Biotech is doing the same to centralized health institutions: returning power to the n = 1 practitioner.
This is the core idea of The Sovereign Individual — considered one of the most prescient works of the late 20th century. It’s also foundational to the broscience practice.

The thesis is simple:
“Technology will make individuals more sovereign than ever before.”
What can this possibly have to do with broscience?
Well let’s start here. Recall our mention of the explosion of experimental anecdotes from a single observation to thousands of testing opportunities:
“technology of mass production has been eclipsed by a new technology of miniaturization. With the new information technology has come a new science of nonlinear dynamics…whose startling conclusions are mere strands that have yet to be woven together into a comprehensive worldview.”
“Mere strands” awaiting to be pieced together into a more “comprehensive worldview”. Sound familiar to n = 1 → 10 → 10,000?
We now have unprecedented access to tools once reserved for elite researchers:
Personalized diagnostics → Services like Superpower (once available only to the top 0.1%) analyze blood biomarkers transforming individual anecdotes into collectively represented data.
Research peptides → Available at a fraction of Big Pharma costs for personal experimentation.
Real-time biofeedback → Wearables like Oura and Whoop track sleep, HRV, & recovery metrics.
Genetic insights → Testing from 23andMe & Nebula Genomics enables tailored interventions: supplement protocols, dietary adjustments, training modifications.
Distributed information networks → Platforms like X & Substack function as thought marketplaces crowdsourcing validation and falsification in real-time. This accelerates the nonlinear growth from N=1 to many.
We place special emphasis on the final piece as it relates directly to the incentive of mutual cooperation across practitioners:
“information technology can accommodate multiple processes at the same time. It disperses activities on networks, allowing for redundancy and substitution between workstations that could number in the thousands or even the millions and be anywhere on earth. In increasing numbers of activities, it is possible for people to cooperate without ever coming into physical contact with one another.”
The incentive structure is self-correcting. The broscientist’s reputation depends on authentic results. Successful self-experimentation compounds into continued success. Otherwise, deceptive & fraudulent behavior is more costly for each player in the game.
Many Cases of “Right Again”
We’ve been saying it for years: “Broscience vindicated again.”
But has this n = 1 self-research approach actually been effective?
Consider these the archetypes of the “bros have been saying this” in recent history:
Preservation of muscle during cutting phases w/ resistance training4 → Bros maintained training intensity while dieting down. Research eventually confirmed muscle retention requires mechanical tension, not just calories.
Varying rep ranges to hypertrophy5 → High reps, low reps, medium reps. Doesn’t matter. All worked in the framework of progressive overload. Science later validated multiple pathways to hypertrophy.
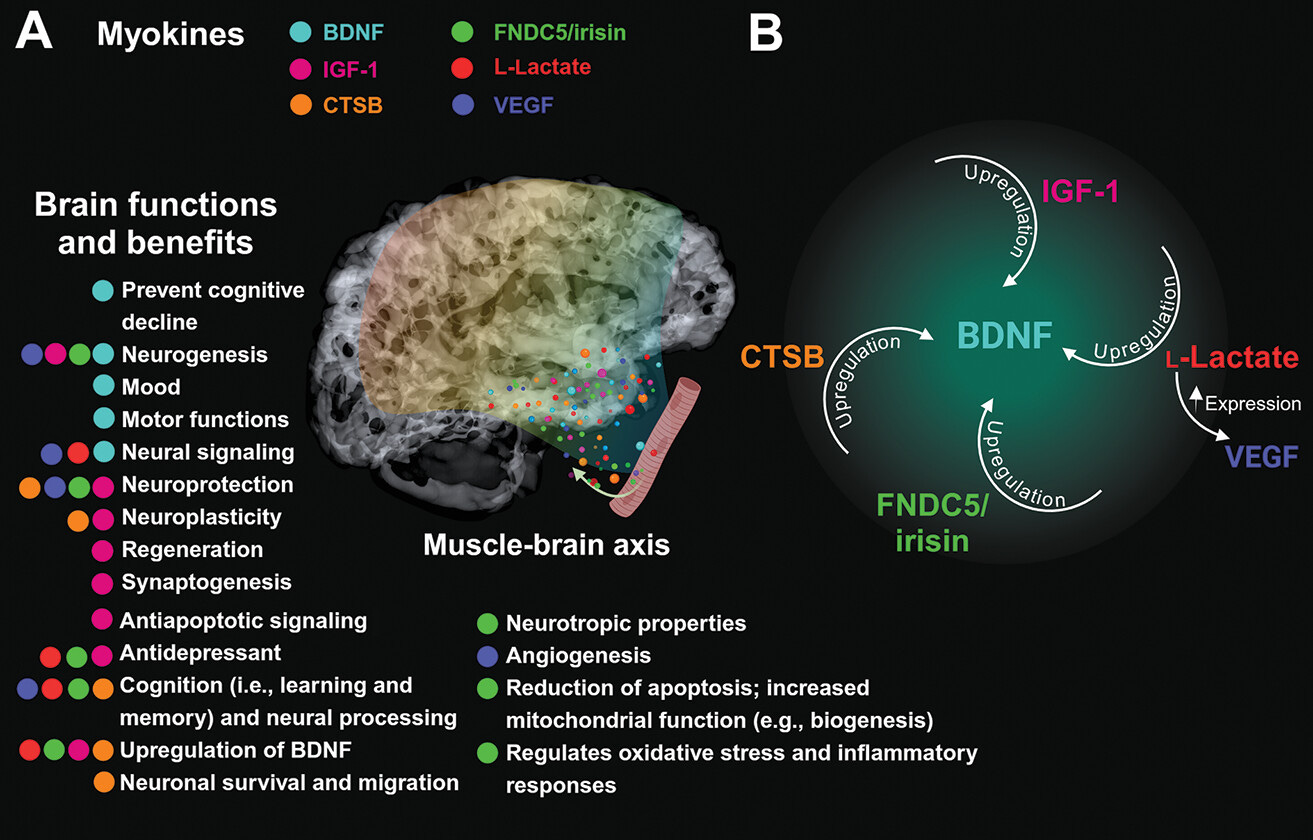
Cognitive benefits of exercise6 → “Lifting makes me feel sharper” became “exercise increases BDNF & neurogenesis.”
Tadalafil as pre-workout tool7 → Vasodilation for pumps. Now studied for exercise performance and cardiovascular function.
Fasted cardio for insulin sensitivity8 → Morning cardio on an empty stomach. Metabolic research is only starting to catch up. (Lifting isn’t cardio. Do your fasted cardio.)
Creatine for cognitive function9 → Not just for skeletal muscle/explosiveness benefits. Brain energy metabolism benefits too.
GLP-1 mimetics for cardiovascular risk reduction10 & metabolic function11 → Bodybuilders experimented years before the word Ozempic was ever spoken. Bros testing retatrutide today remain far ahead.
More protein = fat free mass retention12 → “Eat more protein” was only bro gospel decades before optimal intake studies.
The pattern became clearer than ever in the last 5 yrs: Practitioners observe, experiment, & adjust. Science follows with a mechanistic explanation & validation.
This won’t always be called “broscience”, but the methodology will persist. The vanguard of health optimization will continue operating at the edge of formal research, validating principles through direct experimentation before institutions catch up.
Where Academic Science Falls Short
Subject Selection
Most health and fitness research studies diseased populations: type 2 diabetics, obese individuals, sedentary people. Effect sizes are massive because there’s enormous room for improvement.
If you’re already healthy and optimizing performance, you’re operating near the physiological ceiling. These interventions show minimal or no effect. Academic research optimizes for statistical significance in high-risk populations. Broscience optimizes for what moves the needle when you’re already metabolically elite.
Individual Response Heterogeneity
Roger Williams’ 1956 book Biochemical Individuality remains essential reading. His thesis:
“There is no such thing as a truly “normal” individual meaning average. We are all biochemically unique and need to be dealt with as such.”

RCTs assume uniformity, but individuals vary wildly. Results are averaged out masking the neutral or even negative effects seen within treatment groups. This variability amplifies as someone advances toward the margins of optimization.
Lack of Real-World Context
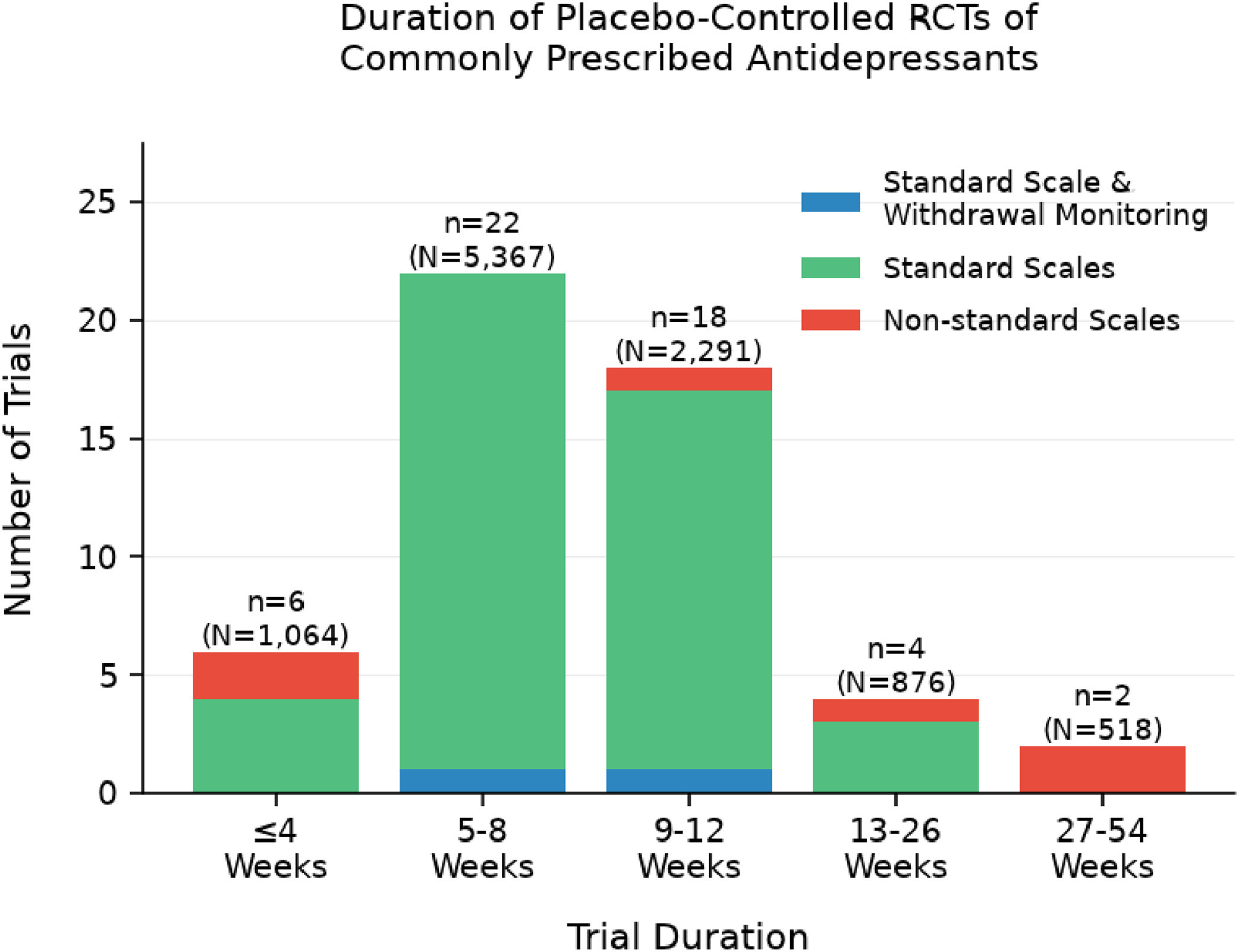
Trials typically run 8-12 weeks, missing long-term consequences. Two of the biggest violations: psychiatry (SSRIs) & hydrogenated vegetable oils (seed oils).
SSRIs → Most RCTs run under 12 weeks13 with none extending past one year. Yet median SSRI use is ~5 years, with 70% of users remaining on them for over 2 years. Twelve weeks isn’t long enough to observe common side effects: sexual dysfunction14, insomnia15, emotional blunting16, & fatigue17.
Seed oils → Mainstream health influencers cite short-term RCTs showing neutral or beneficial effects of high omega-6 oils. These trials miss what happens over time.
Hydrogenated oils flood tissues with polyunsaturated fatty acids (PUFAs), temporarily boosting vitamin E levels while creating long-term imbalance18 —PUFA stores outpace antioxidant half-life. Oxidative stress slowly damages DNA (cancer risk19), lipoproteins (cardiovascular and liver issues20), & proteins (neurological and thyroid harm21). These effects require years to manifest and escalate with age as cumulative oxidative damage compounds. RCTs can’t capture decades of exposure.
Our lives and the interventions we impose on them cannot be compressed into 8-week trials. The practitioner fills this gap by falsifying and validating where trials fall short, especially in domains formal research has never been able to reach until now.
Why “Open-Source” is the Future
Broscience originated in the bodybuilding & fitness spheres decades ago. However the methodology expands into health more broadly today. And what makes this all possible is accessible technology: CGMs, biomarker testing, peptides, & gene therapy.
Over-the-counter CGMs broke regulatory barriers when the FDA approved the first one in 2024. The market is projected to grow from $371 million (2024) to over $1 billion within a decade22. Direct-to-consumer biomarker testing will surge from $1.1 billion (2024) to $2.3 billion (2034)23, with at-home kits delivering lab-quality insights without requiring a doctor’s approval.
As the pendulum swings from centralization to decentralization, medical knowledge is no longer gatekept and dispensed top-down by credentialed authorities. Instead we have distributed experimentation where n=1 researchers armed with consumer-grade diagnostic tools run their own trials.
The future isn’t one vector for us. We fade the reductionist dogma (per usual). It’s the synthesis of broscience & academic science. Academic research remains the gold standard for establishing causality. When we say “the bros were right again,” we’re intrinsically acknowledging that formal science carries weight by it validating or falsifying the anecdotal signal. The future belongs to directional checks and balances between disciplines.
We should remain skeptical of both extremes:
Academic ossification: Researchers clinging to outdated paradigms decades after contradictory evidence emerges. Institutions moving at regulatory pace while real-world experimentation accelerates. The PhD dismissing anecdotal patterns because they lack peer-reviewed blessing.
Broscience charlatanism: Influencers hawking unproven compounds with zero accountability. The n=1 evangelist ignoring confounders. The biohacker nuking their endocrine system chasing vanity metrics.
This is why the solution can be thought of as open-source health with scientific rigor. A decentralized network of self-experimenters feeding data into collaborative analysis platforms.
This is the great health decentralization opportunity happening right before us. A testament to the bright future of our health space. Broscience scaled, systematized, & validated in real-time. Open-source health embedded in a closed-loop control system.
We are living in the greatest time in all of human history.
For the first time ever, the tools to understand and optimize your biology are in your own hands. And that means you’re in control.
The barriers to knowledge have been torn down.
The cost of self-experimentation has collapsed.
The speed of validation has accelerated.
A grassroots health movement unlike any we’ve had in the past. The question isn’t whether this approach will shape the future of our health landscape. It’s whether you will participate in building it.
Stay after it and until next time.
Your friend,
Phys
Meng X, Liu X, Tan J, Sheng Q, Zhang D, Li B, Zhang J, Zhang F, Chen H, Cui T, Li M, Zhang S. From Xiaoke to diabetes mellitus: a review of the research progress in traditional Chinese medicine for diabetes mellitus treatment. Chin Med. 2023 Jun 22;18(1):75. doi: 10.1186/s13020-023-00783-z. PMID: 37349778; PMCID: PMC10288731.
Galen. (1823). De sanitate tuenda. In C. G. Kühn (Ed.), Claudii Galeni Opera Omnia (Vol. 6, pp. 1–452). Leipzig: Knobloch.
Tipton CM. Susruta of India, an unrecognized contributor to the history of exercise physiology. J Appl Physiol (1985). 2008 Jun;104(6):1553-6. doi: 10.1152/japplphysiol.00925.2007. Epub 2008 Mar 20. PMID: 18356481.
Lyngbæk MPP, Legaard GE, Nielsen NS, Durrer C, Almdal TP, Lund MAV, Liebetrau B, Ewertsen C, Lauridsen C, Solomon TPJ, Karstoft K, Pedersen BK, Ried-Larsen M. Effects of caloric restriction with different doses of exercise on fat loss in people living with type 2 diabetes: A secondary analysis of the DOSE-EX randomized clinical trial. J Sport Health Sci. 2024 Oct 18;14:100999. doi: 10.1016/j.jshs.2024.100999. Epub ahead of print. PMID: 39427878; PMCID: PMC11964559.
Cumming KT, Elvatun IC, Kalenius R, Divljak G, Raastad T, Psilander N, Horwath O. Divergent strength gains but similar hypertrophy after low-load and high-load resistance exercise training in trained individuals: many roads lead to Rome. J Appl Physiol (1985). 2025 Sep 1;139(3):685-697. doi: 10.1152/japplphysiol.00353.2025. Epub 2025 Aug 19. PMID: 40827709.
López-Ojeda W, Hurley RA. Myokines and the Brain: A Novel Neuromuscular Endocrine Loop. J Neuropsychiatry Clin Neurosci. 2025 Winter;37(1):A4-4. doi: 10.1176/appi.neuropsych.20240173. PMID: 39812655.
Aversa A, Fittipaldi S, Francomano D, Bimonte VM, Greco EA, Crescioli C, Di Luigi L, Lenzi A, Migliaccio S. Tadalafil improves lean mass and endothelial function in nonobese men with mild ED/LUTS: in vivo and in vitro characterization. Endocrine. 2017 Jun;56(3):639-648. doi: 10.1007/s12020-016-1208-y. Epub 2017 Jan 30. PMID: 28133708.
Liu X, He M, Gan X, Yang Y, Hou Q, Hu R. The Effects of Six Weeks of Fasted Aerobic Exercise on Body Shape and Blood Biochemical Index in Overweight and Obese Young Adult Males. J Exerc Sci Fit. 2023 Jan;21(1):95-103. doi: 10.1016/j.jesf.2022.11.003. Epub 2022 Nov 11. PMID: 36447628; PMCID: PMC9674552.
Marshall S, Kitzan A, Wright J, Bocicariu L, Nagamatsu LS. Creatine and Cognition in Aging: A Systematic Review of Evidence in Older Adults. Nutr Rev. 2025 Sep 13:nuaf135. doi: 10.1093/nutrit/nuaf135. Epub ahead of print. PMID: 40971619.
Jia A, Yang M, Wang T, Hua Y, Lu H. Efficacy and safety of GLP-1 receptor agonists in the treatment of obese patients with chronic heart failure: a meta-analysis. Front Cardiovasc Med. 2025 Oct 3;12:1633114. doi: 10.3389/fcvm.2025.1633114. PMID: 41112222; PMCID: PMC12533278.
Chu J, Zhang H, Wu Y, Huang Y, Zhu T, Zhou Z, Wang H. Efficacy of lifestyle modification combined with GLP-1 receptor agonists on body weight and cardiometabolic biomarkers in individuals with overweight or obesity: a systematic review and meta-analysis. EClinicalMedicine. 2025 Aug 30;88:103464. doi: 10.1016/j.eclinm.2025.103464. PMID: 40926900; PMCID: PMC12414836.
Refalo, Martin C.; Trexler, Eric T.; Helms, Eric R. Effect of Dietary Protein on Fat-Free Mass in Energy Restricted, Resistance-Trained Individuals: An Updated Systematic Review With Meta-Regression. Strength and Conditioning Journal ():10.1519/SSC.0000000000000888, January 22, 2025.
Ward W, Haslam A, Prasad V. Antidepressant Trial Duration Versus Duration of Real-World Use: A Systematic Analysis. Am J Med. 2025 Oct;138(10):1400-1407.e10. doi: 10.1016/j.amjmed.2025.04.037. Epub 2025 May 3. PMID: 40324551.
Bala A, Nguyen HMT, Hellstrom WJG. Post-SSRI Sexual Dysfunction: A Literature Review. Sex Med Rev. 2018 Jan;6(1):29-34. doi: 10.1016/j.sxmr.2017.07.002. Epub 2017 Aug 1. PMID: 28778697.
Wichniak A, Wierzbicka A, Walęcka M, Jernajczyk W. Effects of Antidepressants on Sleep. Curr Psychiatry Rep. 2017 Aug 9;19(9):63. doi: 10.1007/s11920-017-0816-4. PMID: 28791566; PMCID: PMC5548844.
Marazziti D, Mucci F, Tripodi B, Carbone MG, Muscarella A, Falaschi V, Baroni S. Emotional Blunting, Cognitive Impairment, Bone Fractures, and Bleeding as Possible Side Effects of Long-Term Use of SSRIs. Clin Neuropsychiatry. 2019 Apr;16(2):75-85. PMID: 34908941; PMCID: PMC8650205.
Hu XH, Bull SA, Hunkeler EM, Ming E, Lee JY, Fireman B, Markson LE. Incidence and duration of side effects and those rated as bothersome with selective serotonin reuptake inhibitor treatment for depression: patient report versus physician estimate. J Clin Psychiatry. 2004 Jul;65(7):959-65. doi: 10.4088/jcp.v65n0712. PMID: 15291685.
Mariamenatu AH, Abdu EM. Overconsumption of Omega-6 Polyunsaturated Fatty Acids (PUFAs) versus Deficiency of Omega-3 PUFAs in Modern-Day Diets: The Disturbing Factor for Their “Balanced Antagonistic Metabolic Functions” in the Human Body. J Lipids. 2021 Mar 17;2021:8848161. doi: 10.1155/2021/8848161. PMID: 33815845; PMCID: PMC7990530.
Azrad M, Turgeon C, Demark-Wahnefried W. Current evidence linking polyunsaturated Fatty acids with cancer risk and progression. Front Oncol. 2013 Sep 4;3:224. doi: 10.3389/fonc.2013.00224. PMID: 24027672; PMCID: PMC3761560.
Wurm R, Schrutka L, Hammer A, Moertl D, Berger R, Pavo N, Lang IM, Goliasch G, Huelsmann M, Distelmaier K. Polyunsaturated fatty acids supplementation impairs anti-oxidant high-density lipoprotein function in heart failure. Eur J Clin Invest. 2018 Sep;48(9):e12998. doi: 10.1111/eci.12998. Epub 2018 Aug 1. PMID: 30004123; PMCID: PMC6175474.
Cobb CA, Cole MP. Oxidative and nitrative stress in neurodegeneration. Neurobiol Dis. 2015 Dec;84:4-21. doi: 10.1016/j.nbd.2015.04.020. Epub 2015 May 27. PMID: 26024962; PMCID: PMC4662638.
Grand View Research. (2025). CGM market report 2025–2033. https://www.grandviewresearch.com/industry-analysis/continuous-glucose-monitoring-market
Future Market Insights. (2024). At-home biomarker testing market 2024–2034. https://www.futuremarketinsights.com/reports/advanced-at-home-biomarker-testing-market
Great content, thanks for sharing.
As a retina doc, I was just thinking about this topic today. I watched a video of someone suggesting saffron for age-related macular degeneration. I did a quick literature search and learned there there have been a few small RCT’s showing benefit. But ultimately, the conclusion was "we need more studies with longer follow-up and bigger sample size…”
As a doctor, I am reluctant to recommend something to all patients without rigorous RCT data. But let’s be honest, there will never be a large RCT of saffron for eye disease - it would take years and it’s just too expensive. Unless it can be patented, there isn’t a financial incentive to put the resources into a large RCT.
And yet I see patients every day who had a parent go blind from macular degeneration and they ask me desperately, “Is there anything more I can do to prevent it?” I’m struggling with what we as doctors should say. The promotion of N of 1 studies is a potential answer to this dilemma.