

Peptides: What's Real, What's Hype
BPC-157, GLP-1s, the Russian bioregulators, & growth-hormone peptides — Huberman's 2h 48m w/ Dr. Abud Bakri. Distilled into what you can actually use.

The Phys Debrief · #01
The practical takeaways & latest research from the health space's most valuable long-form content, without the rest.
Peptides have officially become a household term.
It was only a matter of time before the biggest names in the health game caught on. And who better to welcome the topic into the mainstream peptide era than the most based doctor on this side of the health space: Abud Bakri MD
Given our immense respect for Abud, we’re kicking off The Phys Debrief series immortalizing his most recent & wildly popular podcast appearance.
Side note: You can manifest things. You can just speak them right into existence. A month-old prediction coming true.

Full episode linked below for your next Zone 2/3 session.
Contents:
In 1 Sentence
In 50 Words
In 250 Words
Practical Takeaways
Episode Blueprint
Where to Listen & Watch
In One Sentence
The most useful way to think about today’s peptide boom is to ask whether a given peptide has a known receptor — GLP-1s do and work predictably, while most everything else (like BPC-157, Russian bioregulators, thymic peptides, GHK-Cu) is promising but rests on animal models, single-lab data, and anecdote, which implies lifestyle fundamentals and clean, physician-monitored sourcing matter more than the molecule itself.
In 50 Words
Peptides are exploding in popularity and poorly understood. Bakri’s lens: known-receptor peptides (GLP-1s) are strong and predictable; no-receptor peptides (BPC-157, bioregulators, thymic peptides, GHK-Cu) are promising but thinly evidenced in humans. Most people buy from an unverified gray market. Foundations first. Physician oversight and reputable sourcing are paramount.
In 250 Words
Bakri’s organizing framework is one question: does a peptide have a known receptor? GLP-1s do, so their effects are strong and consistent. BPC-157, TB-500, and the Soviet-era “bioregulators” don’t (or we haven’t found them…yet), so they likely act by modifying existing proteins or as epigenetic modifiers. And their human evidence is thin.
BPC-157 is the centerpiece. Discovered from gastric juice by one Croatian group (Sikirić’s lab), its impressive healing data is almost entirely animal. It appears to accelerate repair by upregulating angiogenesis, nitric-oxide signaling, and growth-factor activity, which is also why a theoretical cancer concern exists (it could feed an existing tumor). Oral BPC doesn’t seem to reach the bloodstream, but injectable does. Bakri thinks the underexplored gut and neuro effects (gut protection, blunted addiction/stimulant reward) are more interesting than the musculoskeletal hype.
The bioregulators (pinealon, epitalon, vilon) act like transcription-assisting epigenetic modifiers. Huberman reports pinealon dramatically raising his REM fraction. The thymus shrinks from puberty and its decline tracks cancer/autoimmune/cardiovascular risk. A $3 lymphocyte-to-monocyte ratio is a usable proxy almost no clinician checks. GH secretagogues raise your own IGF-1 but worsen insulin sensitivity. GLP-1s are the one category with robust receptor-based human data and are reshaping metabolic medicine.
Nearly all peptide Active Pharmaceutical Ingredients (API) is Chinese and splits into big-pharma, compounding, gray-market, and black-market tiers of wildly varying quality → Wild Wild Peptide West. Get the foundations right first. If you proceed, do it with a peptide-literate physician, objective endpoints, and verified sourcing.
Practical Takeaways
Mental Models (first principles)
Sort any peptide by one question: Does it have a known receptor? Receptor peptides (GLP-1s) produce strong, predictable effects. No-receptor peptides (BPC-157, TB-500, bioregulators) may act via protein modification or epigenetics, but their human effects are largely unproven. As a shortcut, a drug name ending in “-tide” signals a peptide and the root often hints at the mechanism.
Foundations are the floor & peptides are additive on top: AM sunlight, consistent sleep, minimally processed food, and regular training come first. Bakri is explicit: stacking peptides is pointless if the basics aren’t in place.
BPC-157
Calibrate your confidence to the data: Almost all efficacy and safety data is animal and comes from a single Croatian group. Meaningful human data amounts to roughly one small ulcerative-colitis trial. The most-cited “proof” (an Olympic athlete’s Achilles recovery) is hearsay.
Mechanism is pro-repair, not anti-inflammatory: It appears to upregulate VEGF/angiogenesis, nitric-oxide signaling, growth-factor receptor density, and cell migration (especially stacked with TB-500). The same angiogenesis is the basis of the theoretical tumor-vascularization concern, which is exactly why Huberman won’t take it when he isn’t injured.
Route matters: Oral and rectal BPC don’t appear to reach systemic circulation (not detected in blood); injectable does. Most people inject ~100–250 mcg, but Bakri argues the effective human dose is probably far higher. Dosing is guesswork because there’s no human pharmacokinetic data.
The under-discussed effects are gut and neurological: Gut protection (anti-ulcer, anecdotal travel/GI resilience), plus a homeostatic dampening that in animals blunts intoxication and withdrawal — and in some users blunts stimulant/addiction reward (reported “blunted Adderall,” low mood/anhedonia).
“PDA” is BPC-157: Compounded “pentadecapeptide arginate” is the same molecule in a different salt. The current legal workaround as FDA compounding status shifts.
Bioregulators (pinealon / epitalon)
The naming is backwards: Pinealon (tripeptide EDR) comes from cortex extract, not the pineal. Epitalon (AEDG) is the pineal one. Both behave like transcription-assisting epigenetic modifiers with no known receptor.
Timing flips pinealon’s effect: Morning or pre-workout, it’s an anti-fatigue/cognitive tool. High doses near bedtime can fragment deep sleep. Huberman’s anecdote: a small dose taken on a mid-night waking sharply increased his REM fraction with lingering benefit on subsequent nights.
Watch blood sugar and expect vivid dreams: Pinealon modulates metabolic and antioxidant pathways (PPAR-α/γ, SOD, GDF11, irisin). Some users see blood glucose (& HbA1c) drop. Use extra caution if hypoglycemia-prone. Intense, unusually vivid dreams are common.
Epitalon is interesting because it targets repair machinery, not a downstream receptor: Animal data span retinal degeneration (retinitis pigmentosa, glaucoma models) and restoration of melatonin rhythm in aged animals.
The peptide space has become the Wild Wild West of the health world.
In a category this unregulated, inside a health movement getting more decentralized by the day, I refuse to gamble on anything less than the highest-quality tools.
That’s why I’ve been using YourProtocol. Every batch is 3rd-party lab tested for purity and made in an FDA-registered, GMP-certified facility. They’ve built their reputation on proof and became my only source for oral BPC and bioregulators.
Restore BPC: what I used to heal my gut lining last year.
PinealON: for clear, focused cognition when the stress load piles up.
EpitalON: for deeper sleep and the long game on recovery and longevity.
Don’t take my word for it. Check the lab tests and reviews yourself.
Pick up your protocol (& use PHYS10 at checkout for 10% off your next order).

Thymus & Immunity
The thymus is a longevity-relevant organ, not vestigial: It shrinks from puberty (driven by sex hormones and corticosteroids), and its decline tracks rising cancer, autoimmune, and cardiovascular risk. Removing residual thymus during cardiac surgery carries a measurable mortality signal.
Use the cheapest immune-aging proxy you already have: The lymphocyte-to-monocyte ratio from a standard CBC with differential (~$3) tracks outcomes across many diseases. Aim for robust lymphocytes (~1,500–3,000) with low monocytes. Almost no clinician looks at it.
Know the thymic peptides apart: Thymosin α1 is pro-immune (Bakri self-experiments with ~2.5 mg twice weekly as travel/hospital prophylaxis — not an approved use). TB-500 is a synthetic Thymosin β4 fragment (and a known doping agent, especially equine). Thymalin (Russian peptide mixture) is not Thymulin (the French zinc-dependent nonapeptide). Thymulin requires adequate zinc; falling thymulin is the earliest marker of zinc depletion.
GHK-Cu
Strongest evidence is topical for skin: This copper tripeptide (Gly-His-Lys) sits in type-1 collagen, is high in youth, and both builds and remodels collagen. Topical human data on photoaging is reasonable (roughly comparable to retinol/vitamin C). Hair data is weak as it’s not a minoxidil replacement and at best an adjunct.
Use it with a routine and pair with red light: GHK-Cu and red-light therapy appear synergistic for collagen/photoaging. A legitimate product should be blue (from the copper). Don’t inject it into your face.
Growth Hormone Secretagogues
These raise your own GH/IGF-1 rather than injecting GH: GHRH-type (sermorelin, tesamorelin) vs. ghrelin/GHRP-type (ipamorelin, MK-677). MK-677 drives large, non-pulsatile GH and the most appetite and side effects. Tesamorelin + ipamorelin can push IGF-1 to puberty-range levels.
There are trade-offs: GH and secretagogues worsen insulin sensitivity (A1c rises). The bodybuilding maxim is “get lean enough to run GH”. The open question is promotion of an existing cancer, not initiation. Huberman tried sermorelin: it boosted deep sleep, suppressed REM, and spiked his PSA — he stopped immediately.
GLP-1s
This is the one category with strong, receptor-based human data: It’s reshaping metabolic medicine (10–30% body-weight loss). The class originated from Gila-monster peptide. Retatrutide (a GLP-1/GIP/glucagon triple agonist) is the next wave.
Titrate slowly and pair with lifestyle (”training wheels”): Many reported negatives (like low mood, fatigue) track with under-eating, low electrolytes/protein, and crashed blood sugar from mega-dosing, not necessarily the drug itself. Bakri’s own 1 mg cold-start produced a night of projectile vomiting. Don’t cold-start high.
Mind the second-order effects: Microdosing under monitoring at the lowest effective dose is the sane approach. Fertility can rebound as obese/anovulatory women lose weight and leptin normalizes (”Ozempic babies”). GLP-1s are not contraception.
Sourcing & safety
Understand the supply chain: Nearly all peptide API is Chinese. It then splits into big-pharma (most stringent), compounding pharmacies (variable), gray-market “research use only” (unknown identity, dose, and batch-to-batch consistency), and black market (avoid entirely). Gray market is how most people actually buy.
Ask your prescriber the markup question: Ask what the compounding pharmacy charges them vs. what they’re charging you. The spread often goes to the clinician, a practice of dubious legality. And no malpractice carrier covers non-FDA-approved injectable peptides.
If you proceed, do it right: A peptide-literate physician, objective monitoring (e.g., IGF-1 on secretagogues), and verified sourcing. The likely near-term future is physician-led telehealth that drives prices down and surfaces which compounders are reliable.
Episode Blueprint
[00:00:00–00:06:26] Introduction & What Peptides Are
Key Points
Huberman frames the “celebrity protocol”: stacking a GLP-1, a GH modulator, and androgen therapy to transform body composition fast as the cultural backdrop.
Bakri’s core taxonomy: peptides are a cellular communication “language” sitting between steroid hormones and full proteins. The key split is known-receptor vs. no-receptor.
GLP-1s have clear receptors (strong, consistent effects). BPC-157 and TB-500 have no identified receptor.
“Peptides are one of the languages of the human body.”
— Dr. Abud Bakri
[00:06:26–00:19:27] BPC-157: Discovery, Mechanism & Neuro/Gut Effects
Key Points
Origin story: Pavlov’s gastric-juice work + Hans Selye’s stress-damage observations led a Croatian group (1991) to isolate the 15-amino-acid BPC-157 from a larger gastric protein. We don’t natively make BPC-157. We make the parent protein.
Animal work: faster healing of severed tendons/ACL, protection against burn-induced gastric ulcers. The Achilles paper is what ignited athlete interest.
Proposed mechanism is pro-repair: VEGF/angiogenesis, nitric-oxide signaling, more growth-factor receptors, cell migration and it preserves healing even alongside corticosteroids.
Bakri finds the neuro/gut effects more compelling than musculoskeletal: animals get “less drunk,” withdraw less severely, and some users report blunted stimulant reward via the gut-brain axis.
“The original idea of BPC was a gastric treatment, not musculoskeletal.”
— Dr. Abud Bakri
Studies referenced
A new gastric juice peptide, BPC (Journal of Physiology-Paris, 1993) — Frames BPC as a gastric-juice peptide that protects organs against stress-induced damage; the conceptual root of BPC-157 (Sikirić group).
BPC 157 accelerates healing of transected rat Achilles tendon (Journal of Orthopaedic Research, 2003) — In rats and tendon-cell culture, BPC-157 sped healing of a fully severed Achilles tendon; the result that drove athlete interest.
Achilles detachment in rat and BPC 157: tendon-to-bone healing, opposed corticosteroid aggravation (Journal of Orthopaedic Research, 2006) — BPC-157 improved tendon-to-bone healing and counteracted corticosteroid-impaired healing; basis for the “pro-repair, not anti-inflammatory” claim.
[00:19:27–00:29:41] BPC-157: Adverse Events, Trials & Legality
Key Points
No known LD50 (animals tolerated ~1,000× doses), which itself blocks FDA approval.
Human data ≈ small phase 1/2 rectal-enema trials for ulcerative colitis (~80 mg) from the same Croatian group (abstracts only, full data unavailable). Orally/rectally administered BPC wasn’t detectable in blood.
Legality is shifting and state-dependent: BPC-157 was never FDA-approved → moved to a “do-not-compound” list in late 2024 → then off it in 2025. Compounded “PDA” is the workaround. Telehealth law follows the patient’s state.
“All the animal data come from one group.”
— Dr. Abud Bakri
[00:29:41–00:41:32] The Peptide Market: Compounding, Gray & Black Market
Key Points
The GLP-1 shortage pushed people to compounding pharmacies and gray-market “research only” sites. Injecting became normalized, which de-stigmatized peptides broadly.
Nearly all API is Chinese. Quality runs from excellent to dreadful, batch to batch, with no way for the buyer to verify.
More than half the peptide market is women (GHK-Cu, skin/collagen). Affiliate selling exploded.
“The best job in 2025 was to be a peptide affiliate.”
— Dr. Abud Bakri
[00:41:32–00:54:19] Tumor/Angiogenesis Risk; Patents & Designing a Real Trial
Key Points
The honest worry: BPC-157’s angiogenesis could vascularize an undetected tumor. No human signal exists, but there’s also no good human data and in some models it actually decreased VEGF (e.g., a melanoma line).
Patents are weak (add one amino acid and it’s a “new” compound). The original patent passed to Teva, which has no incentive to develop it.
A sensible trial program: finish the colitis work (encapsulated, not enema), test GERD vs. pantoprazole, and study tendon-repair endpoints (e.g., post-surgical bicep/ACL recovery time).
“Both of those are very bad endpoints.”
— Dr. Abud Bakri (on access vs. harm)
[00:54:19–01:07:25] BPC-157 Anecdotes; Physician, FDA & Malpractice
Key Points
Bakri’s grade-2 tricep tear (normally ~3-month recovery) healed in 3–4 weeks with local high-dose injection plus other peptides. Huberman’s acute neck/trap pull resolved in 2 days after ~200 mcg. Both stress these are uncontrolled anecdotes.
Dosing online is set by “what fits in the vial,” not data.
Patients can sue the physician, the pharmacy, and the recommender. No malpractice carrier covers non-FDA-approved injectables. The right model is a frank physician-patient discussion with monitoring and clear endpoints.
“What the hell are you doing? This is healing so fast.”
— Dr. Abud Bakri’s physical therapist
[01:07:25–01:29:38] Bioregulators: Pinealon/EDR & Epitalon
Key Points
Pinealon (EDR) derives from cortex extract. Epitalon (AEDG) from the pineal — the names mislead. Both act like epigenetic modifiers that help expose promoter regions of DNA.
Pinealon improves daytime cognition/anti-fatigue (Khavinson’s athlete studies) and raises REM fraction with lingering effects. Watch for blood-sugar drops and vivid dreams.
Epitalon targets DNA-repair machinery relevant to retinal degeneration and melatonin-rhythm restoration. Khavinson’s framing: replenishing youthful peptides that decline with age, with benefits that accrue even when off-cycle.
“It is a whole other life to get that much REM.”
— Dr. Andrew Huberman
Studies referenced
Pinealon increases cell viability by suppressing free radicals and activating proliferation (Rejuvenation Research, 2011) — In neuronal/cell models, pinealon raised viability by lowering free-radical levels. Mechanistic support for the “better oxidative state” story, not human sleep data.
[01:29:38–01:50:33] Thymus, Thymosin α1, TB-500, Thymulin & Pets
Key Points
The thymus shrinks from puberty under sex hormones and corticosteroids. Lower thymic function tracks worse outcomes across diseases. Fahy’s TRIIM trial regrew it with GH + metformin + DHEA.
Thymosin α1 (pro-immune; FDA-approved abroad/for congenital athymia as Zadaxin) used by Bakri as travel prophylaxis. TB-500 = Thymosin β4 fragment (actin/cell migration; equine doping agent).
Thymalin (Russian peptide mix) ≠ Thymulin (French zinc-dependent nonapeptide that augments end-organ hormone responses and requires adequate zinc).
Veterinary openness to peptides is high. A large “pet peptide” market is emerging.
“We don’t have thymologists.”
— Dr. Abud Bakri
Studies referenced
Health consequences of thymus removal in adults (New England Journal of Medicine, 2023) — Adults who had the thymus removed showed higher all-cause mortality and cancer risk; the residual adult thymus still matters.
Thymic health consequences in adults (Nature, 2026) — In a human MRI cohort, higher thymic scores tracked lower cardiovascular and cancer mortality; supports thymic function as a measurable longevity metric.
Reversal of epigenetic aging and immunosenescent trends in humans (TRIIM trial) (Aging Cell, 2019; Fahy et al.) — A 12-month GH + metformin + DHEA cocktail regrew thymic tissue and reversed epigenetic-age estimates; proof-of-concept, small and uncontrolled.
Chemical characterization of thymosin β4 (Journal of Biological Chemistry; Goldstein lab) — Characterized the thymosin β4 peptide, the parent of TB-500.
Human whole-blood NAD+ levels do not vary with age or lifestyle interventions (Nature Metabolism, 2026) — Whole-blood NAD+ didn’t decline with age or shift with lifestyle interventions. Complicates the “boost NAD for longevity” narrative behind NMN/NR (raised in the same tangent).
[01:50:33–02:04:01] GHK-Cu & a $3 Immune-Aging Blood Test
Key Points
GHK-Cu (Gly-His-Lys + copper) sits in type-1 collagen, declines with age, and both synthesizes and remodels collagen. Discovered by Loren Pickart. Topical skin data is reasonable, but the hair data is weak.
Illness recovery: every infection causes transient thymic atrophy. Chronic stress prevents rebound, leaving people repeatedly sick.
Practical tool: the lymphocyte-to-monocyte ratio on a routine CBC is a cheap, ignored proxy for immune robustness and disease risk.
“A $3 lab test that everybody gets and no one looks at.”
— Dr. Abud Bakri(paraphrased)
Studies referenced
Protective effects of GHK-Cu in bleomycin-induced pulmonary fibrosis (Life Sciences, 2020) — In an animal fibrosis model, GHK-Cu reduced fibrosis via anti-oxidative/anti-inflammatory pathways; basis for emerging (preclinical) interest in lung/COPD/long-COVID regeneration.
[02:04:01–02:15:36] Growth Hormone Secretagogues
Key Points
Secretagogues raise endogenous GH/IGF-1: GHRH-type (sermorelin, tesamorelin) vs. ghrelin/GHRP-type (ipamorelin, MK-677). MK-677 produces the largest non-pulsatile GH and most side effects.
Somatopause (GH decline in the 30s) is the target; the debate is whether replacing it helps or harms longevity (GH-deficient models often live longer; antagonistic pleiotropy).
GH worsens insulin sensitivity and may promote existing tumors; Huberman’s sermorelin trial spiked his PSA and suppressed REM.
“You have to get lean enough to take growth hormone.”
— Dr. Abud Bakri
[02:15:36–02:20:25] GHK-Cu Topical + Red Light
Key Points
Best results: a well-formulated topical (should be blue) used alongside a normal skincare routine, not instead of it.
GHK-Cu and red/near-IR light appear synergistic for collagen and photoaging. Sunlight is the original full-spectrum source.
“Use it with the rest of your skincare, not in place of it.”
— Dr. Abud Bakri (paraphrased)
Studies referenced
Longer wavelengths in sunlight pass through the body and improve vision (Scientific Reports, 2025) — Red/near-IR wavelengths penetrate the body and exert systemic effects, including on vision. Context for the GHK-Cu + red-light synergy and “sunlight is the best source.”
[02:20:25–02:39:03] GLP-1s & Retatrutide
Key Points
The class (from Gila-monster peptide) is transforming metabolic medicine; without it the system would buckle under obesity/diabetes. Robust receptor-based human data sets it apart.
Long-term/cognitive effects of thousand-fold GLP elevations are unknown. Reported mood/energy issues often trace to under-eating and electrolyte/blood-sugar problems rather than the drug.
Retatrutide (39 amino acids) is being positioned as a biologic (longer patent protection, harder to compound). Nomenclature is a mess — “peptide” is too broad to be a useful category (carnosine and retatrutide are both peptides).
“There is no pre-GLP-1 world for us anymore.”
— Dr. Abud Bakri
Studies referenced
Early onset of reproductive function in female mice treated with leptin (Science, 1997; Chehab et al.) — Leptin accelerated onset of reproductive function in female mice. Mechanistic backdrop for the fertility rebound (”Ozempic babies”) as body fat and leptin normalize.
[02:39:03–02:48:00] Women’s Reproductive Disorders, TBI & Safe Sourcing
Key Points
No animal or human data supports BPC-157 or similar for endometriosis/fibroids. Those are hormonal/metabolic problems where the hormonal lever is far stronger.
TBI: Russian work on cortexin and cerebrolysin exists but won’t be US-available. BPC’s neuro effects are homeostatic (”won’t let the brain go too far in either direction”).
Where to get peptides safely: not gray-market sites; build a relationship with a peptide-literate physician, monitor objective endpoints, and expect physician-led telehealth to improve sourcing and price over 6–24 months.
“You have no choice but to get educated.”
— Dr. Abud Bakri (to physicians)
Listen & Watch (on 0.75x speed…IYKYK)
YouTube:
Spotify:
Where to find Dr. Bakri:
Here on Substack: Abud Bakri MD
Pair this together with our peptide history timeline & you place yourself in the top 1% of knowledge in this space.

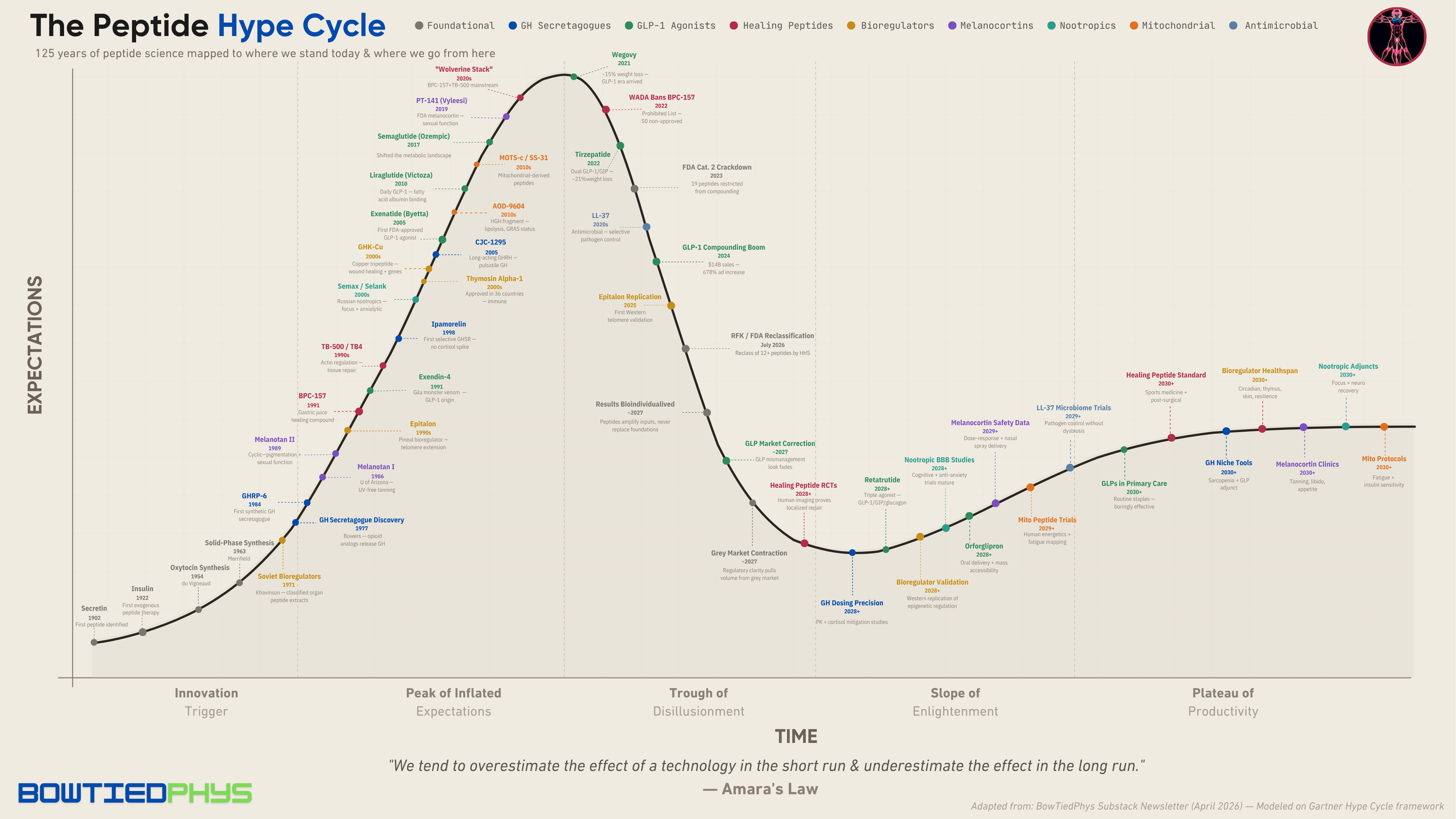
Downloadable PDF plot below for detailed viewing (abridged version):
And we’ll be talking a lot more about these in the near future.
Stay after it until then.
Your friend,
Phys
Top podcast from Huberman! Everyone should listen and watch.
When you are thinking about peptides, where you you go to find research peptides? I found a site that lists all of the different peptide companies and they do not sell peptides but they have links to vendors with rating. https://findpeptides.org/product is a very interesting site if you are looking to purchase grey market peptides.