

The Glycine Paradox: When Your Sleep Supplement Becomes Your Stimulant
Maybe you don't need to be glycine maxxing

You did everything right. Took the magnesium. Took the 3 grams of glycine an hour before bed. And now it’s 2 AM. The monkey brain is louder than it was at noon, and you’re punching into Perplexity “why does glycine keep me awake”.
It’s neither your imagination nor another Reddit-induced symptom. The same molecule that sedates most is exciting your neurons through a receptor system few know of.
Here’s why that’s happening & a ranked protocol to fix it.
Contents:
How Glycine Promotes Sleep
Why Glycine Wires Some People Up
The Four Factors Behind the Paradox
The Protocol: Ranked by Priority & ROI
How Glycine Promotes Sleep (When It Works)
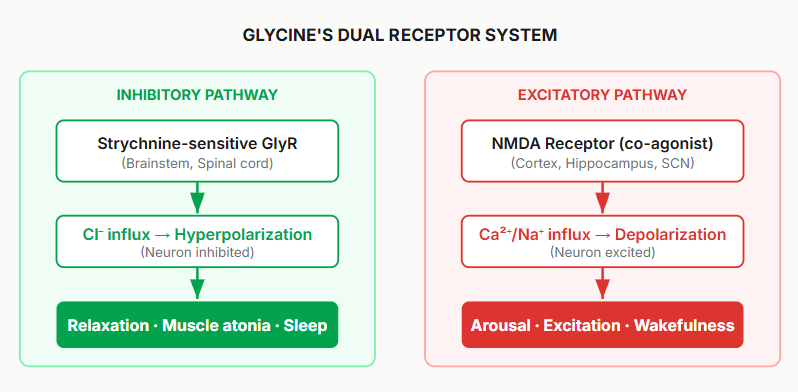
Glycine is one of two inhibitory neurotransmitters in the central nervous system — GABA being the other. Its functions range from glutathione synthesis to bile acid conjugation to neurotransmission and is a big reason why you hear so much chatter on eating nose-to-tail in the social media space.
Glycine activates NMDA receptors triggering the thermoregulatory cascade that initiates natural sleep: peripheral vasodilation → drops core body temperature → shortens sleep onset latency.
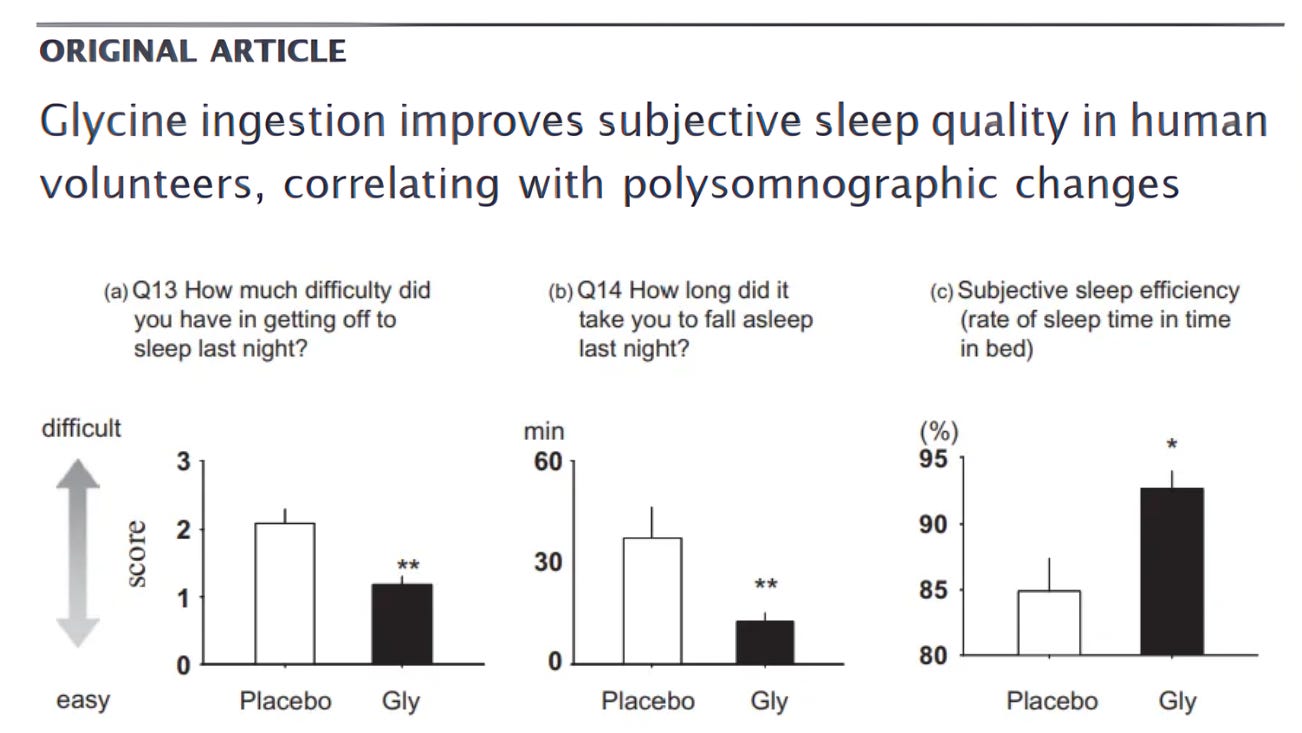
In Yamadera et al. (2007), 3 g of glycine taken one hour before bedtime:
Improved subjective sleep quality
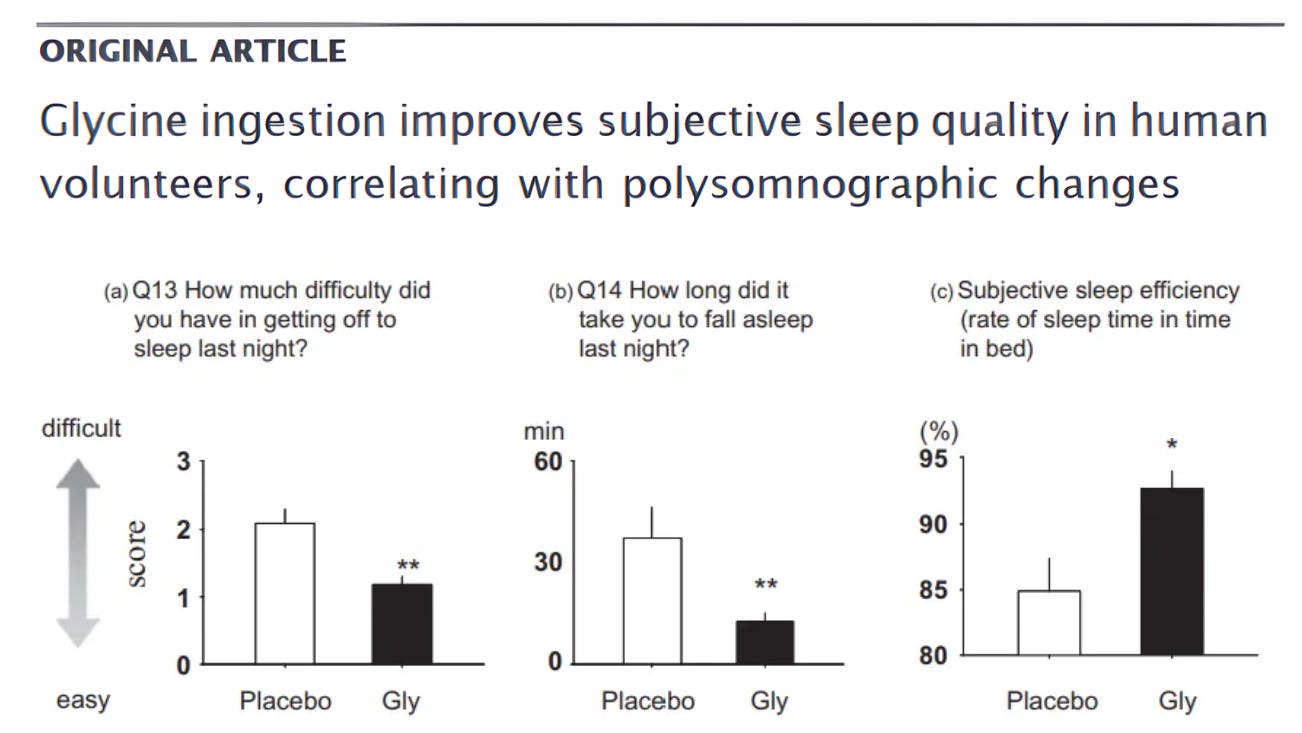
Shortened sleep onset
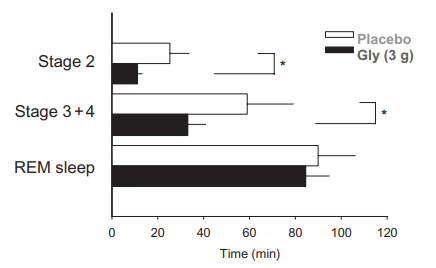
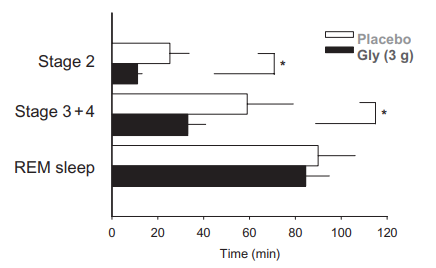
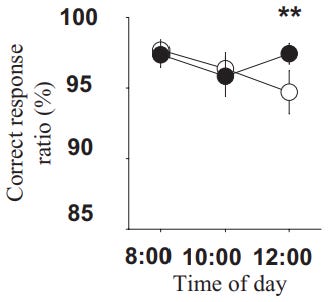
Effects of glycine (Gly) on the latency to sleep stages Improved next-day cognitive performance
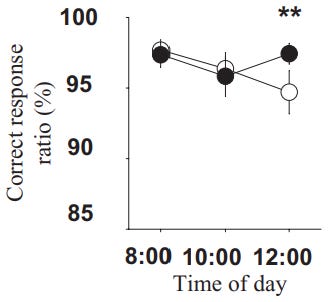
Effects of glycine (Gly) on memory recognition task
But unfortunately, there’s biochemical variation (many such cases).
The Paradox: Why Glycine Wires Some People
Glycine acts as an inhibitory neurotransmitter, but it also functions as a co-agonist with glutamate at the NMDA receptor’s glycine binding site.
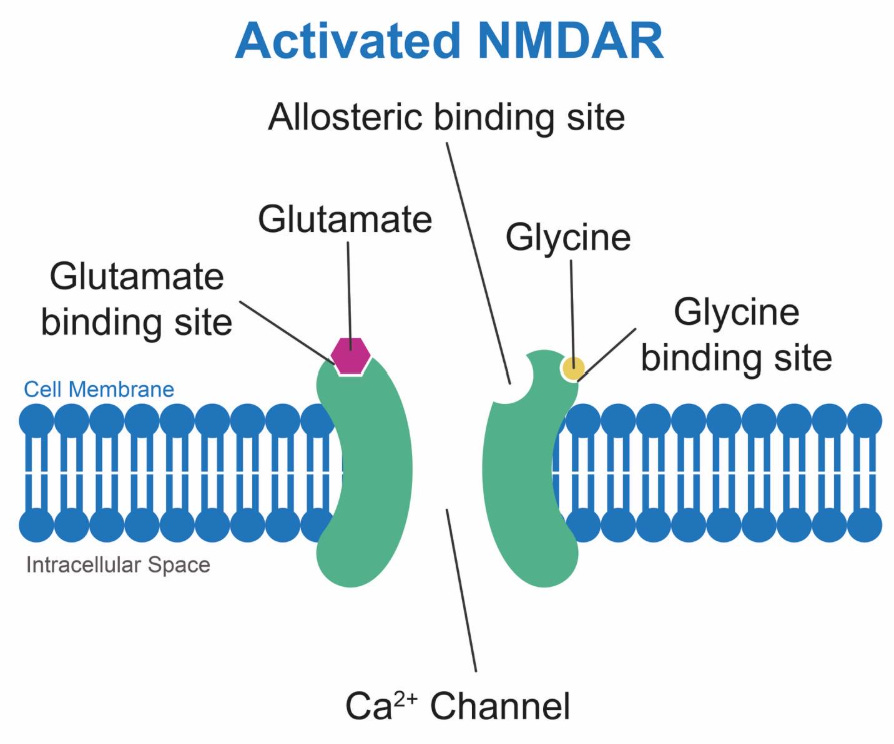
By taking exogenous glycine, you saturate both the inhibitory glycine receptors & the NMDA co-agonist site. And the latter mechanism is how you start to activate glutamatergic excitation across the brain.
Zhang et al. (2014) showed this switch is dose-dependent & bidirectional:
Low extracellular glycine → favors long-term NMDA depression → net inhibition + calmer brain
Higher glycine → flips to long-term NMDA potentiation → strengthened excitatory synapses + heightened arousal
The same molecule that zonks one person out in 30 min leaves another staring at the ceiling at 2 AM with monkey brain, night sweats, & a heart rate that won’t drop below 75 bpm.
That’s the glycine paradox summed up. And where you fall on that spectrum comes down to four predisposing factors.
The Four Factors Behind the Paradox
1. Impaired Cellular Energy Metabolism (The Master Variable)
GABA & glycine normally inhibit neurons by opening chloride channels allowing chloride ions to flow in and create a calming negative charge. But this requires low intracellular chloride levels maintained by the KCC2 transporter.
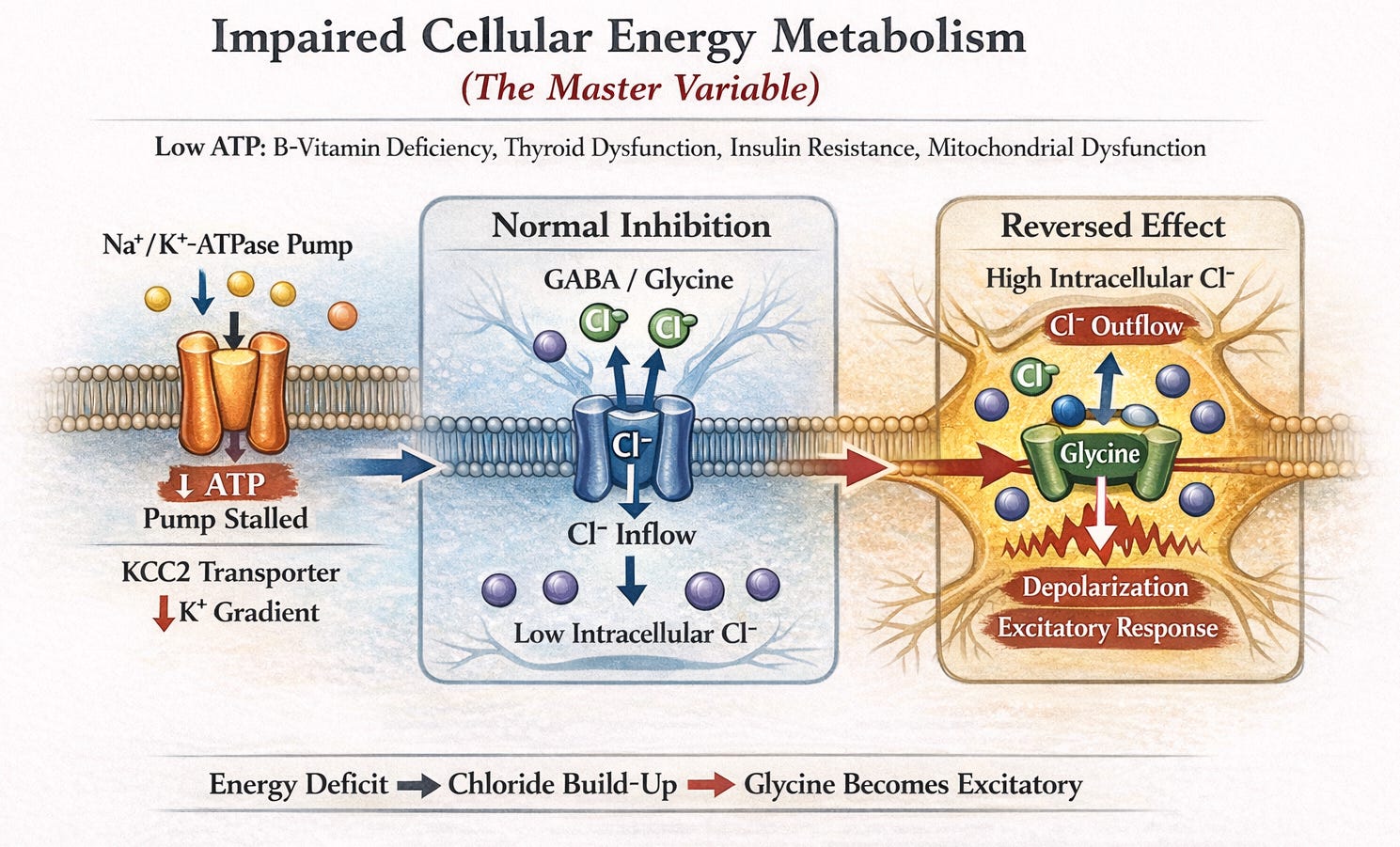
KCC2 relies on a potassium gradient generated by the Na⁺/K⁺-ATPase pump, which consumes ATP to function properly. When ATP levels drop due to factors like B-vitamin deficiencies, thyroid/mitochondrial issues, or insulin resistance, the pump fails leading to chloride buildup inside neurons.
Opening the channels causes chloride to flow outward depolarizing the cell and flipping glycine (and potentially GABA) from inhibitory to excitatory.
This is why both creatine (increased phosphocreatine stores) & niacinamide (a direct NAD+ booster) can rescue glycine intolerance: it restores ATP → rebuilds the chloride gradient → flips the switch back to calm.
2. Elevated Glutamate Tone / GABA-Glutamate Imbalance
NMDA receptors need both glutamate and glycine to fire. If your glutamate tone is already elevated (anxiety, MSG in hyperpalatable foods, glutamine supps, neuroinflammation), glycine simply completes the circuit unbalancing your inhibitory-to-excitatory signaling.
Glutamine converts to glutamate in the brain via glutaminase. It’s a great tool for fortifying the gut barrier (especially for the elite athletes here), but it can easily be a hidden trigger. More on that later.
3. Genetic & Epigenetic Vulnerabilities
For those who’ve done genetic testing, certain variants tilt the scales toward excitation:
GLRA1/GLRB: Weaker inhibitory glycine receptors.
GlyT1/GlyT2: Slower glycine clearance, prolonging NMDA exposure.
MTHFR: Impaired methylation and ATP production; glycine itself feeds into this loop.
GAD1/GAD2: Poor glutamate-to-GABA conversion, especially with low B6.
4. Environmental & Lifestyle Factors
If your system is already wired for excitation (poor daylight exposure + bright evenings via blue heavy LEDs/screens + excessive nnEMF), bringing glycine into the picture floods NMDA sites & furthers excitatory signaling.
The Protocol: Ranked by Priority & ROI
The interventions below are ordered by mechanistic importance and expected return on investment. Start at the top and work down. Most will resolve the issue within the first three tiers.
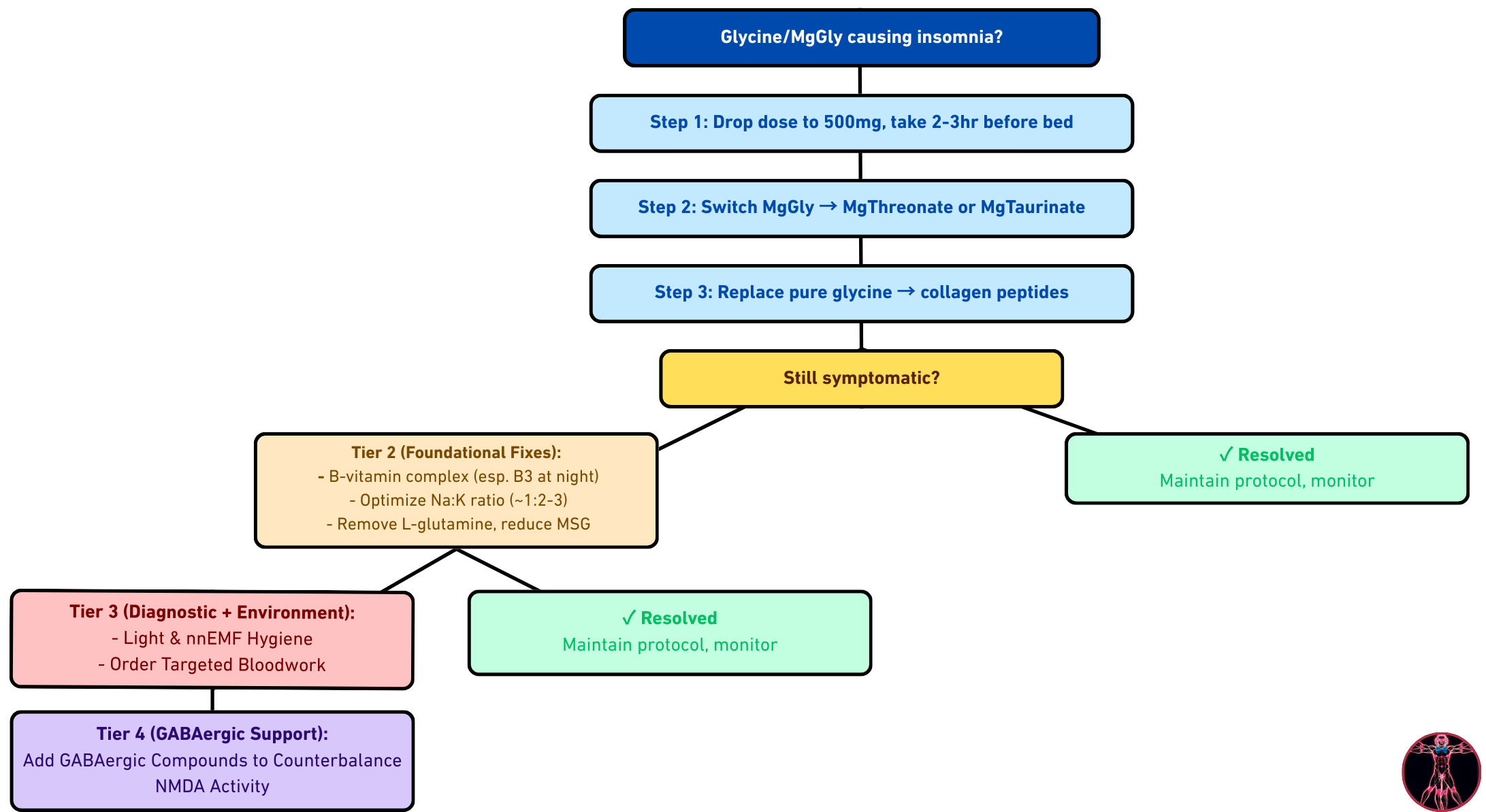
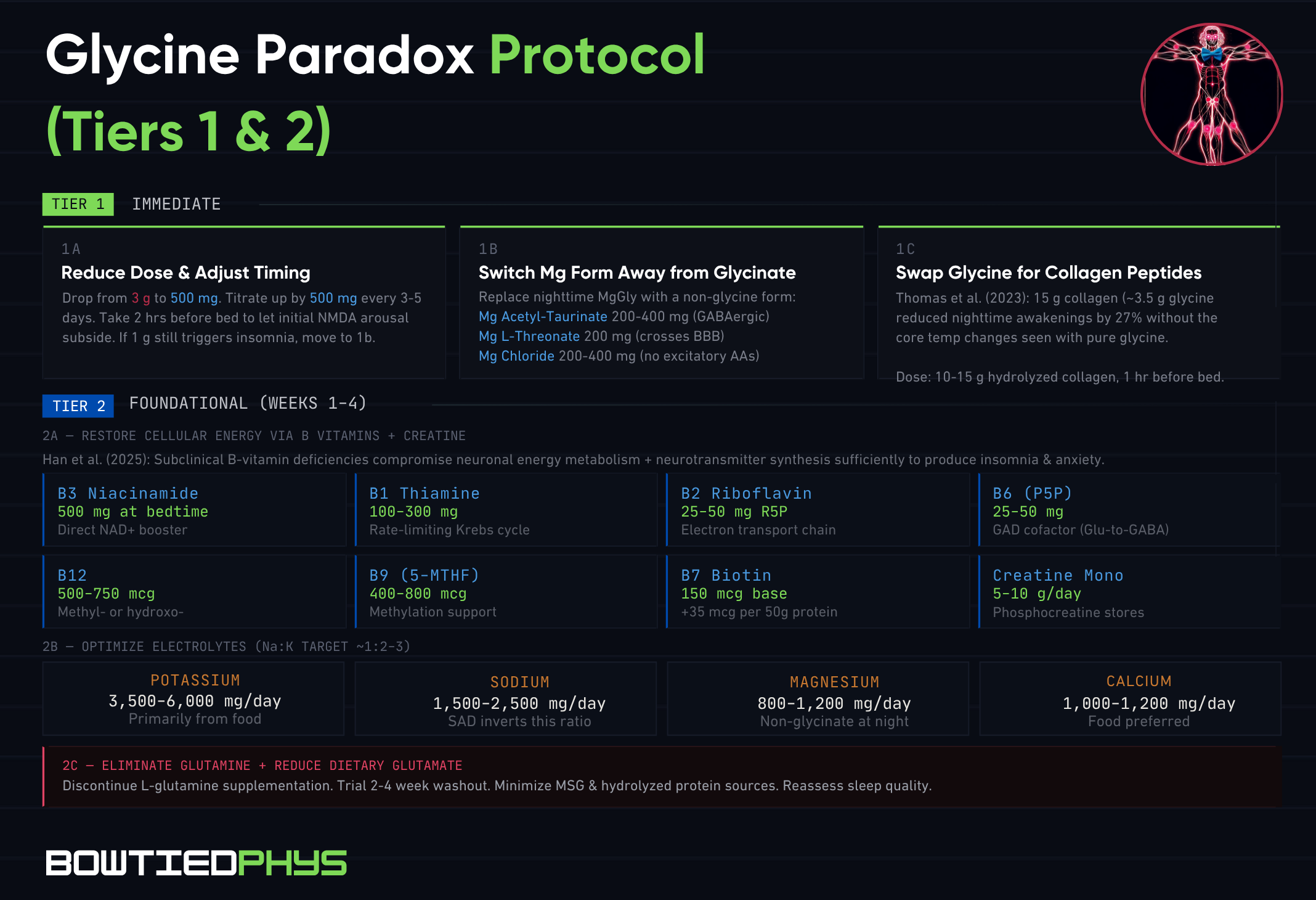
Tier 1 — Immediate
1a. Reduce Dose & Adjust Timing
Drop from 3 g → 500 mg & titrate up by 500 mg increments every 3–5 days. Take glycine after dinner (2–3 hours before bed) rather than at bedtime giving time for the initial NMDA-mediated cortical arousal to subside.
Dose: Start at 500 mg, 2–3 hrs before bed. Titrate to tolerance. If 1 g still produces insomnia, move to intervention 1b.
1b. Switch Magnesium Form Away from Glycinate
Replace magnesium glycinate with a non-glycine form for your nighttime dose. Reserve glycinate for daytime if desired.
Forms (ranked):
➜ Magnesium acetyl-taurinate (200–400 mg Mg; taurine adds GABAergic support)
➜ Magnesium L-threonate (200 mg Mg; crosses BBB, supports synaptic Mg²⁺)
➜ Magnesium chloride (200–400 mg Mg; well-absorbed, no excitatory amino acids).
1c. Swap Isolated Glycine for Collagen Peptides
Thomas et al. (2023) showed that 15 g collagen peptides (providing ~3.5 g glycine) reduced nighttime awakenings by 27% without the core temperature changes seen with pure glycine.

Dose: 10–15 g collagen peptides (hydrolyzed, grass-fed bovine or wild-caught marine), 1 hr before bed, dissolved in liquid without food.
Tier 2 — Foundational (Weeks 1-4)
2a. Restore Cellular Energy Metabolism via B Vitamins + Creatine
Han et al. (2025) noted that subclinical deficiencies in B1, B2, B3, B6, folate, & B12 compromise neuronal energy metabolism and neurotransmitter synthesis sufficiently to produce insomnia, anxiety, and cognitive dysfunction.
Priority B vitamins:
➜ B3 (Niacinamide): 500 mg at bedtime.
➜ B1 (Thiamine): 100–300 mg benfotiamine or thiamine HCl. Rate-limiting for Krebs cycle.
➜ B2 (Riboflavin): 25–50 mg riboflavin-5'-phosphate. Supports electron transport chain.
➜ B6 (P5P): 25–50 mg. Cofactor for GAD enzyme (glutamate → GABA).
➜ B12: 500—750 mcg methylcobalamin or hydroxocobalamin. Check serum B12 on next bloods.
➜ B9 (5-MTHF): 400–800 mcg. Supports methylation.
➜ B7 (Biotin): 150 µg for first 100 g protein + every additional 50 g protein requires an extra 35 µg biotin.
Track intake via Cronometer, Microgram or any micronutrient tracking app.
2b. Optimize Electrolytes (Sodium, Potassium, Magnesium, Calcium)
Target a sodium-to-potassium ratio of ~1:2–3 by intake. The sad story of SAD (Standard American Diets) is inverted (high sodium + low potassium = cardiovascular issues).
Targets:
➜ Potassium: 3,500–6,000 mg/day (primarily from food)
➜ Sodium: 1,500–2,500 mg/day
➜ Magnesium: 800–1,200 mg/day (food + supplement, non-glycinate form at night)
➜ Calcium: 1,000—1,200 mg/day (food preferred)
2c. Eliminate Glutamine Supplementation & Reduce Dietary Glutamate
If you are supplementing L-glutamine for gut related use cases, trial a 2–4 week washout & assess sleep quality changes. Eliminate all hyperpalatable foods high in added glutamate.
Action: Discontinue L-glutamine. Or at least, prioritize around breakfast. Minimize MSG & hydrolyzed protein sources. Reassess after 2–4 weeks.
Tier 3 — Diagnostic + Environmental
3a. Order Targeted Bloodwork
Test. Don’t guess.
Priority labs on next bloodwork:
➜ Serum B12 + methylmalonic acid (functional B12 status)
➜ Full thyroid panel: TSH, free T3, free T4, reverse T3, TPO antibodies (thyroid dysfunction = impaired ATP)
➜ Fasting insulin + glucose (poor insulin sensitivity = impaired neuronal energy)
➜ Homocysteine (elevated = impaired methylation, B12/folate/B6 functional status)
➜ RBC magnesium (serum Mg is unreliable; RBC reflects intracellular stores)
➜ Serum ferritin (iron is cofactor for SHMT enzyme interconverting glycine)
Optional (if above is unrevealing):
➜ Organic acids test (OAT): screens for B vitamin functional deficiencies, mitochondrial dysfunction
➜ MTHFR / COMT / GAD1 genotyping: leverage if there's a pattern of paradoxical supplement responses
3b. Light & EMF Hygiene
Blue-light blockers post-sunset, dimming lights to <50 lux in the evening (incandescents), and minimizing social media time/digital exposure 45—60 min before bed can significantly reduce the excitatory load that glycine is being added on top of.
Actions:
➜ Blue-light blockers (red ones) after sunset
➜ Dim ambient light to <50 lux after 8 PM
➜ Device-free wind-down period 45—60 min before bed
➜ Kill nnEMF sources (phone/router)
Tier 4 — GABAergic Support (Add as Needed)
4a. Add GABAergic Compounds to Counterbalance NMDA Activity
Evidence-based GABAergic agents (ranked by strength of evidence):
Amino acids & related compounds:
➜ Taurine (3–5 g): Activates GABA-A & glycine receptors. Calms neural excitability without binding NMDA.
➜ L-Theanine (400–800 mg): Upregulates brain GABA. Structurally similar to glutamate so competitively inhibits glutamate binding at AMPA receptors.
➜ Myo-inositol (2–4 g): Involved in GABA-A receptor function via phosphoinositide signaling. Evidence for anxiolytic & sleep-promoting effects at higher doses.
Herbal GABAergics:
➜ Lemon balm (300–600 mg extract): Inhibits GABA-transaminase (the enzyme that degrades GABA) raising synaptic GABA levels. Reduced insomnia by 42% as standalone in one trial.
➜ Passionflower (250–500 mg extract): GABA-A positive allosteric modulator via chrysin and other flavonoids. Comparable to oxazepam (30 mg) for generalized anxiety in one RCT.
➜ Valerian root (300–600 mg extract): Contains valerenic acid, a GABA-A positive modulator.
➜ Chamomile (200–400 mg extract): Apigenin binds GABA-A benzodiazepine site with moderate affinity.
➜ Magnolia bark (200–400 mg): Contains honokiol & magnolol, potent GABA-A positive allosteric modulators with anxiolytic & sedative properties.
➜ Lavender/Bergamot (aromatherapy): Modulates voltage-dependent calcium channels and GABA-A receptors.
➜ Baikal Skullcap (250–500 mg): Baicalein & baicalin compounds modify the GABA-A receptors
Glycine Insomnia: Step-Through Protocol
SUMMARIZED

Alright that’s a wrap for this week. Sleep deeply.
Your friend,
Phys