

Stop asking "cut or bulk?"
Start reading the 30+ signals that decide it


Every 3–4 months, the same health topics get recycled across the major social platforms. Last week it was another classic.
Should the skinny fat dude cut or bulk?

Only fitting we give it a proper analysis.
I couldn’t care less whether he should put on size or cut down first. I’m focused on what nearly every quote post and reply missed: what factors should determine the path for you.
A focus on the variables that matter and a nuance-heavy counter to the reductionism of short-form content.
The mirror test is fine as a proxy, but it’s a single input. And it’s one that’s become increasingly distorted by our online generation comparing our own backstage selves to everyone else’s front-stage selves — a cocktail for chronic inadequacy.
The result is a deep delusion: social media-induced body dysmorphia of unprecedented levels.
Let this be the antidote to that.
What’s the point of cutting anyways?
Before hitting the should you question, let’s address why we even do it in the first place because it’s easy to lose the plot.
How Not to Run a Cut
The body-dysmorphic culture has psyop’d a tremendous amount of dudes into believing the goal of a deficit phase is to do your best Machinist impression.

If you’re not stepping on a bodybuilding stage:
Avoid the extreme low levels. For most men, that starts below 10% body fat, and the lower you push beyond that, the more you’ll start to feel like sh*t.
Never cut > 1% body weight/week. All this does is wreck physical & cognitive performance. The logbook will reflect…among many others things.
Keep fats within 20–30% of total calorie range on average. Use the lower end when you refeed / need more carbs for training performance. Use the upper end especially when libido & mood are starting to take a hit.
Violate these three rules & expect a typical pattern to develop:
☒ Libido nosedives.
☒ Testosterone tanks.
☒ Morning wood vanishes.
☒ Legs feel like cinder blocks.
☒ Afternoon energy levels crash.
☒ Thyroid function dysregulates.
☒ Irritability hits an all-time high.
☒ Immune function & training recovery suck.
☒ LDL-C & apo(B) skyrockets (as compensation).
All of this is your body sending signals: “you have better things to focus on than your drive, mood, sexual & hormonal function – go figure out that energy deficit problem first. Until then, the foot is off the gas & we’re going into preservation mode.”
Ask how I know…yes — I am hypocritical here. But I do it for the love of the game & the ability to speak from a personal experience. We f*ck around & find out just so we can figure it out better.

The Protective Nature of Subcutaneous Fat
Up until a certain point, subcutaneous fat is actually a *protective* metabolic organ.
Yes, really.
Subcutaneous thigh fat acts as a metabolic sink. It soaks up circulating fatty acids before they get stored in your liver, muscle, or pancreas instead.
Dip below a certain level & those metabolic benefits diminish.
Why We Cut
The whole point of trimming body fat before a gain phase is to enhance fuel partitioning & metabolic flexibility.
And that means…?
Holding excess fat (especially visceral fat) drives insulin resistance – when your cells stop responding cleanly to insulin’s signal. The nutrients you eat get shuttled toward fat storage instead of muscle. A proper cut limits that.
As you lose fat, you restore insulin sensitivity. The same calories start flowing preferentially toward lean tissue and muscle/liver glycogen rather than fat stores.
All this allows for is an improved anabolic response and more efficient ability to stack lean mass in the future.
The Factors
3 Governing Principles
Think in systems & ratios
Contextualize everything. Avoid single value metrics. No cut/bulk decision should ever be based on a single assessment. Use what’s available to you and what makes sense cost-wise for you.
Establish your own elite baseline ASAP
As you get older, having a baseline of what your highest potential “good” feels & looks like becomes more critical. Get your baselines down across these below measures as soon as possible. It’s never too late.
Every marker is relative to your baseline.
A weak HRV, free testosterone level, or insulin sensitivity for you is probably good for someone else. What matters is the direction and rate of change against your own history. There’s one competition worth focusing on — it’s last week vs. this week you. That’s it.
Category 1: Quantifiable Biomarkers
A. Body Composition
Body Fat %
✔ Ideal target: 10–12% (< 10% becomes net negative)
✔ Method honesty: DEXA = gold standard. Calipers = just need skilled hands. InBody scale = add 3–5% of whatever is returned (InBody is generous) + fine as a directional tool.
✔ Cut if ≥ 15% | Bulk at 10% w/ strong markers elsewhere
Waist-to-Height Ratio
✔ Ideal target: < 0.45
✔ Why it matters: Most cost-efficient visceral-fat proxy there is (a tape measure).
✔ Cut if pushing past 0.5 as weight rises → mass is being added….just the wrong kind.
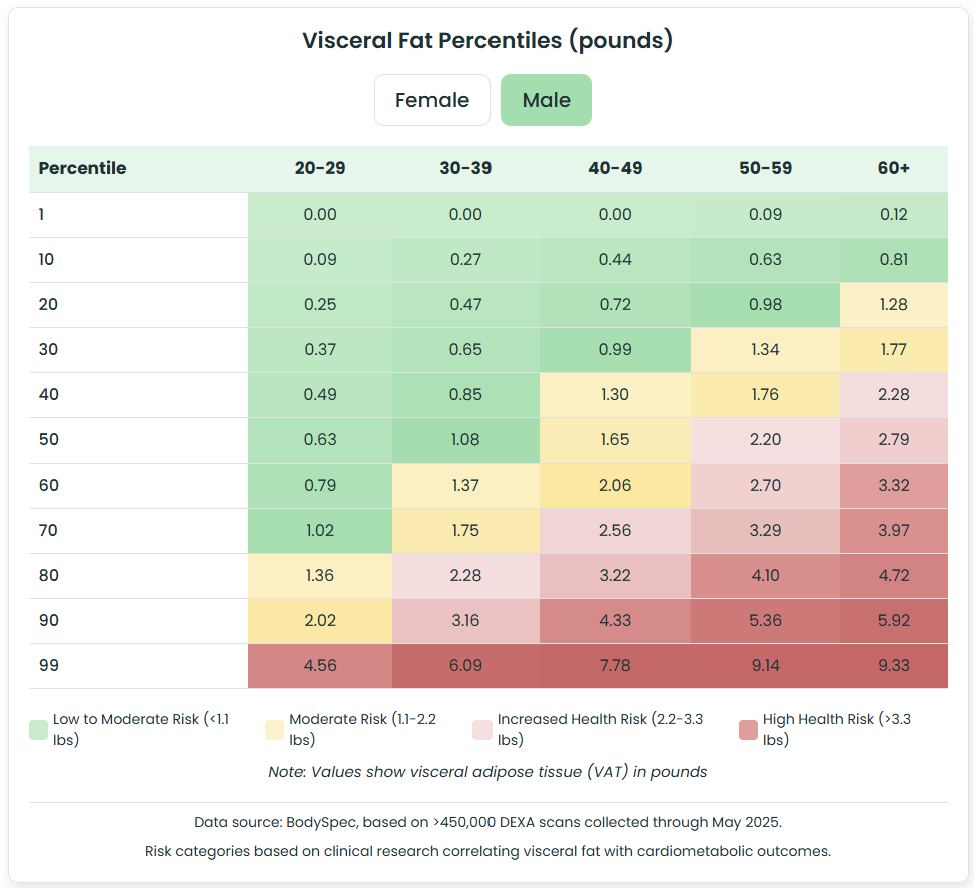
Visceral Fat
✔ Ideal target: DEXA VAT < 0.25 lb (use waist-to-height as your proxy if you can’t get a DEXA)
✔ Why it matters: Primary driver of leptin/insulin sensitivity. High VAT behind even a lean-ish physique is the dominant skinny fat marker.
✔ Cut if elevated regardless of what the mirror test suggests. VAT is a cut signal even at a decent BF %.
Android-to-Gynoid Ratio (Regional Fat Distribution)
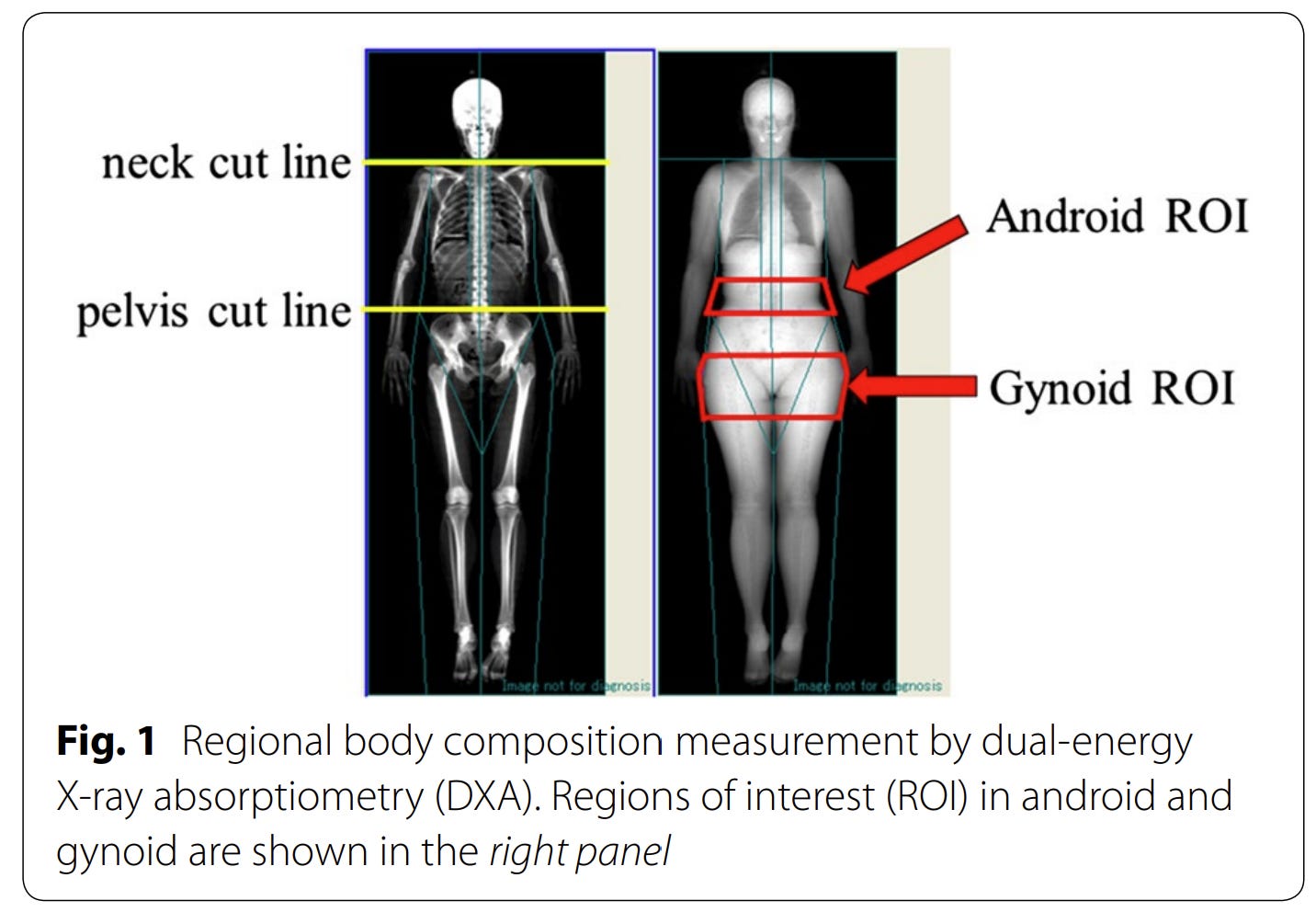
✔ Ideal target: Well-balanced peripheral storage = android (midsection) vs. gynoid (hips/thighs) ratio leaning low (~0.6–0.9)
✔ Why it matters: Where fat is stored reflects hormonal & metabolic status → ab-dominant points to a visceral/cortisol/insulin problem. A higher ratio at low BF usually means a low T-to-E2 ratio. The A/G ratio also tracks closely with visceral fat levels.
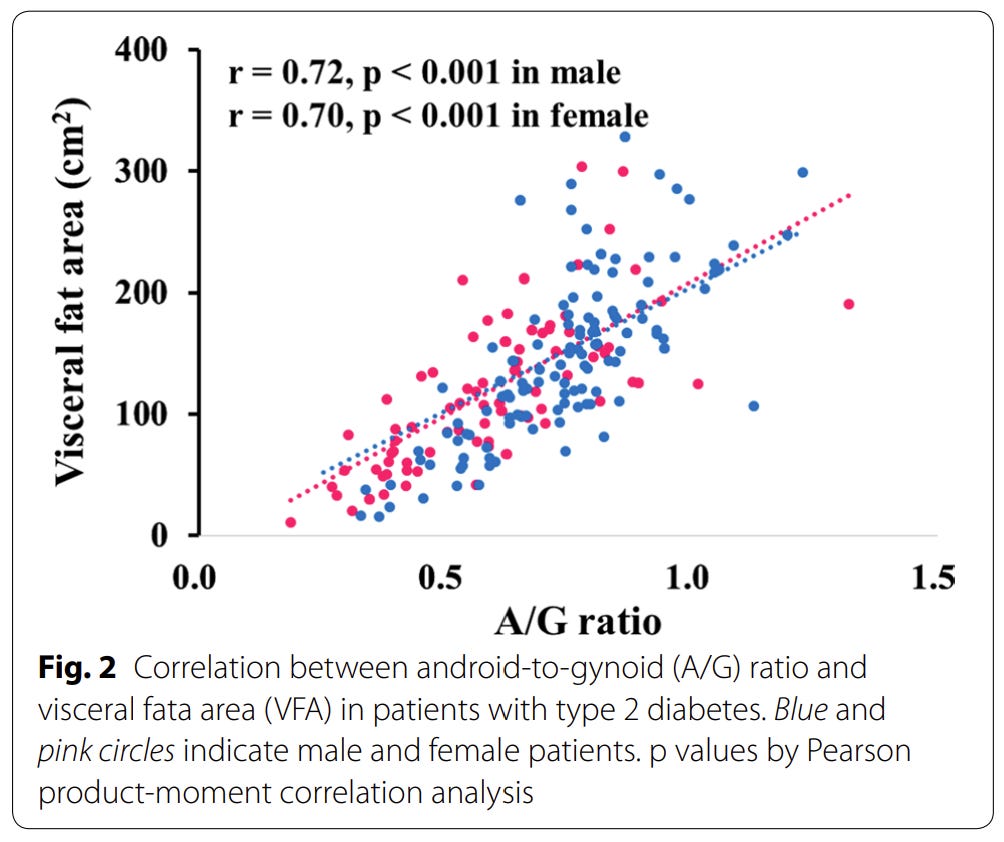
✔ Cut if android-dominant. Additional context: if regional fat persists at otherwise lean BF → look upstream to hormones — Cluster C
Rate of Weight Change
✔ Optimal: Lean gain = 0.25–0.5% BW/week up | Controlled cut = 0.5–1% BW/week down
✔ Why it matters: Another underrated indicator. Cut too quickly → nuke libido/mood/androgen levels. | Bulk too quickly → pile on excess subcutaneous/visceral fat stores (without the additional logbook benefit).
✔ Adjust if faster up (excess fat) or faster down (muscle loss)
Fat-Free Mass Index (FFMI)
✔ Optimal: ~22–24 = well-developed natural | ~25 = natural ceiling
✔ How to calculate:

✔ Bulk if low FFMI with modest body fat→ runway and frame to fill
What this cluster tells you:
✔ Leans CUT → BF > ~15% + waist-to-height > 0.5 + visceral fat > 0.5 lb + scale weight rises faster than ~0.5% BW/week
✔ Leans BULK → BF sitting in the 10–12% zone + visceral fat < 0.25 lb + waist-to-height < 0.45 + FFMI ~18–24
✔ Common trap → Identical-looking physiques can vary significantly. A lean guy with a low FFMI has opportunity to grow. A skinny-fat guy at the same weight with a high waist-to-height usually needs to recomp or cut first.
B. Metabolic
Blood biomarkers measuring fuel partitioning status— most critical cluster for this entire decision.
Triglyceride / HDL ratio
✔ Ideal target: < 1.0
✔ Why it matters: S-tier proxy for insulin sensitivity.
✔ Cut if > 2.0 → priority is to improve fuel partitioning since it’s shifted toward a storage tendency.
Fasting Insulin
✔ Ideal target: 2–5 µIU/mL
✔ Why it matters: Earliest indicator of cardiometabolic state. Flags high insulin resistance 8–10 yrs before glucose budges.
✔ Cut if moving past ~6–8 µIU/mL → cells are losing insulin sensitivity → nutrients partitioning to fat.
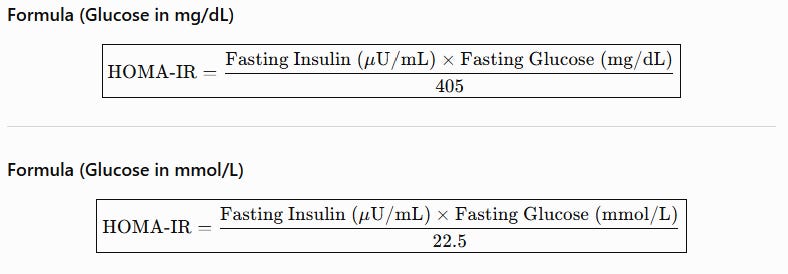
HOMA-IR
✔ Ideal target: < 0.8
✔ Why it matters: Combines fasting insulin + blood glucose into the most validated insulin-sensitivity index.
✔ Cut if > 1.5 → Indication of poor leptin sensitivity & carrying more fat than your cells can handle.
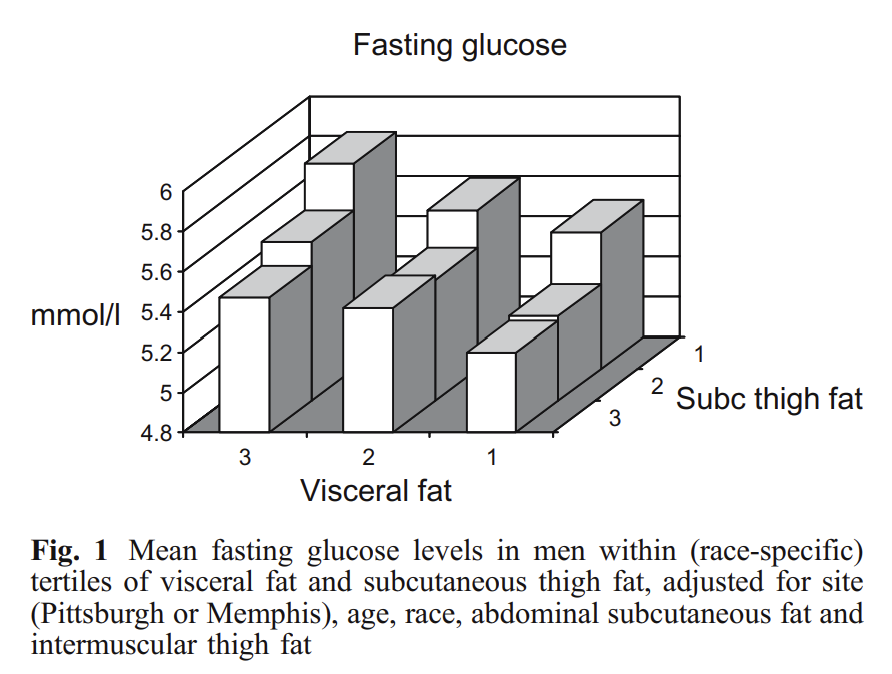
Fasting Glucose
✔ Ideal target: 75–85 mg/dL
✔ Why it matters: Cheap & on every basic metabolic panel, but a lagging signal. Use in context. Will stay normal well after insulin sensitivity weakens.
✔ Cut if consistently > 95–100 (especially paired w/ elevated fasting insulin)
HbA1c
✔ Ideal target: < 5.2%
✔ Why it matters: 3-month glucose average.
✔ Cut if > 5.4% → Chronic glycemic load too high. Always interpret alongside HOMA-IR & Trig/HDL ratio as it can read mildly elevated in very lean, high-RBC-turnover athletes.
CGM-Derived Glucose Variability
✔ Ideal target: A gradual gradient, stable curve. Most readings 70–120 mg/dL. Minimal spikes > 140.
✔ Why it matters: Only marker here showing your real-time response to actual meals and training. A nice tool to experiment with different carb sources at least once – Dexcom G7 is one I’ve had great success with.
✔ Cut if frequent large spikes + slow returns to baseline (glucose intolerance under your current load).
What this cluster tells you:
✔ Leans CUT → Fasting insulin > 6 + HOMA-IR > 1.5 + TG:HDL > 2.0 + high glucose variability widening. Represents a storage-dominant, insulin-resistant state. Caloric surplus at this point adds fat.
✔ Leans BULK → Fasting insulin 2–5 + HOMA-IR < 0.8 + TG:HDL < 1.5 + stable CGM readings. Maximized insulin-sensitive. Green light for a surplus. Exact state where fuel partitioning is locked in & calories drive lean tissue growth.
✔ Common trap → A skinny fat can look lean-ish and still have pre-diabetic metabolic biomarkers = fasting insulin of 12 + HOMA-IR of 2.5. This requires a cut/recomp despite not looking fat. On the other hand, a bigger lean-mass athlete with elite cardiometabolic markers will have set better conditions to bulk than his body comp stats may suggest.
C. Hormonal
Tells you whether you’ve already cut too far or have room to push.
Total Testosterone
✔ Ideal target: 700–1,100 ng/dL for a young male (20–35 yrs) → 700 = ideal floor & 600 = hard stop
✔ Why it matters: Nosedives under chronic energy deficit.
✔ Increase refeed frequency if dropping below 700. Stop cutting if below 600. Excess deficit puts male sex hormones on preservation mode.
Free Testosterone
✔ Ideal target: 18–25 ng/dL
✔ Why it matters: More meaningful than total T. Bioavailable fraction reaching androgen receptors. Can be low even when total looks fine if SHBG is high.
✔ Stop cutting if low despite acceptable total. Common pattern = cutting too quickly → high-SHBG signature → low bioavailable T.
SHBG
✔ Ideal target: ~20–40 nmol/L
✔ Why it matters: Rises with aggressive cutting (> 1.0% of BW). Binds up free T more easily.
✔ Flag if elevated + rising during a cut. Bioavailable T is getting drained.
Estradiol (Sensitive E2)
✔ Ideal target: 20–35 pg/mL (sensitive assay)
✔ Why it matters: Reflects aromatization of testosterone. Too low is associated with reduced libido, easily irritated mood, joint discomfort, impaired recovery, & decreased anabolic signaling. Often declines during prolonged energy restriction as testosterone falls.
✔ Stop cutting / increase calories if falling below ~20 pg/mL alongside declining testosterone. Suggests endocrine suppression from insufficient energy availability.
Testosterone / Estradiol Ratio
✔ Ideal target: 20–35 : 1 (using Total Testosterone [ng/dL] ÷ Estradiol [pg/mL])
✔ Why it matters: A solid T level with disproportionately high E2 usually means excess aromatization. A high ratio during a cut often means E2 falling faster than testosterone. The ratio should always be interpreted alongside the individual hormone values.
✔ Flag if the ratio rises quickly. Common trend among healthy men on extreme cuts is both T & E2 dropping, but E2 proportionally more leading to a ratio rise → indicates that energy availability is becoming too low rather than an improvement in androgen status.
LH & FSH
✔ Ideal target: 2–6 IU/L
✔ Why it matters: LH = stimulates testosterone production. FSH = supports sperm production. Distinguishes why T is low → low LH + low T = your brain has throttled the signal (energy-deficit driven) = “cut too hard” indication.
✔ Stop cutting if low LH + low T. Indicates centralized suppression from low energy availability. Slowly reverse out of the deficit.
Free T3, TSH, Free T4
✔ Ideal targets:
➜ Free T3 = 3.5–4.5 pg/mL
➜ TSH = 0.8–2.0 mIU/L
➜ Free T4 = 1.2–1.6 ng/dL
✔ Why it matters: Earliest endocrine adaptation to a sustained energy deficit is a free T3 drop → downregulates to conserve energy in a deficit.
✔ Stop cutting if Free T3 falling + low afternoon energy + constantly cold + flat feeling during training.
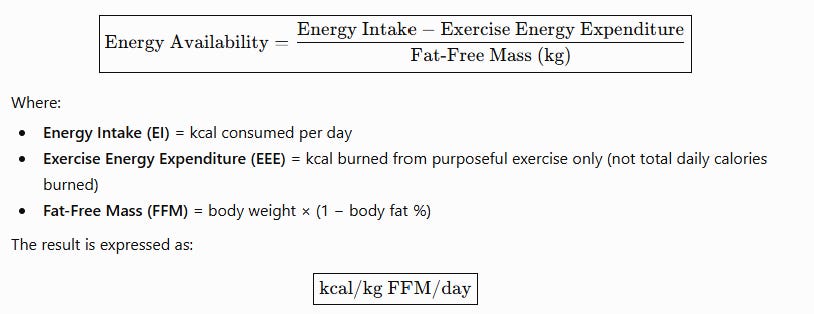
Energy Availability (EA)
✔ Ideal target: > 45 kcal/kg fat-free mass/day → avoid dropping below 30 for more than 5-day period
✔ Why it matters: One of the easiest, most underrated values to guide a bioindividualized deficit period. Upstream cause behind most of this cluster tanking.
✔ Stop cutting if chronically < 30 (RED-S territory). Energy availability falls → hormones tank next → drastic decreases in performance & recovery follows.
What this cluster tells you:
✔ Leans STOP CUTTING / REFEED → EA < 30 + total T < 700 ng/dL + free T < 15 ng/dL + rising SHBG + LH suppressed + Free T3 < 3.0 pg/mL. Represents preservation mode. The deeper the hole, the harder the dig out.
✔ Leans ROOM TO CUT or BULK → EA > 45 + total T > 700 ng/dL + free T > 15 ng/dL + LH/FSH 2–8 IU/L + Free T3 3.5–4.5 pg/mL
✔ Common trap → Low androgen levels get blamed on age, genetics, or minutiae factors. Go upstream first before leaning on TRT – circadian regulation + sunlight + poor sleep efficiency + allostatic load + thyroid status + gut function + possibly self-inflicted energy deficit (or excess body fat). A lean, over-trained, heavily deficit’d guy with low T typically needs to rule out energy availability before touching exogenous hormones/peptides.
D. Lipids & Cardiovascular
Contextualize among metabolic biomarkers always – great indicators on whether you’re too deep in a deficit or carrying excess fat.
ApoB
✔ Ideal target: < 80 mg/dL (optimal < 60 for long-term arterial aging)
✔ Why it matters: Best marker of atherogenic particle burden. More predictive of cardiovascular risk than LDL-C alone.
✔ Cut if elevated alongside high TG + low HDL (the insulin-resistance dyslipidemia pattern → metabolic cut needed)
LDL-C
✔ Ideal target: 70–100 mg/dL
✔ Why it matters: Meaningful only in context. Don’t get fixated on this one. Always interpret alongside ApoB, Trig/HDL, & metabolic biomarkers.
✔ Flag if persistently >120 mg/dL while bulking. Prioritize improving micronutrient-dense food selection, sunlight exposure, increasing food-first fiber intake, movement after meals, and reducing the combined high fat/high carb meals (Standard American Diet) before adding more calories.
HDL-C
✔ Ideal target: > 55 mg/dL
✔ Why it matters: Declines as body fat, leptin/insulin resistance, chronic inflammation, & metabolic stress increase. Falling HDL during a bulk = early sign of fat gain outpacing lean mass gain.
✔ Cut if chronically low (<45 mg/dL) + high TG (>100 mg/dL)
Triglycerides
✔ Ideal target: < 80 mg/dL
✔ Why it matters: The most diet-responsive lipid. Worsens when calories exceed your ability to store nutrients efficiently.
✔ Cut if consistently >120 mg/dL. High triglycerides means poor fuel partitioning & metabolic inefficiency.
hs-CRP
✔ Ideal target: <1.0 mg/L
✔ Why it matters: Marker of systemic inflammation. Needs to be taken into context. High values could mean excess body fat gain, poor recovery, inadequate sleep efficiency, or overtraining.
✔ Investigate alongside other metabolic/hormonal markers before continuing either cut/bulk periods if consistently >2.0 mg/L.
What this cluster tells you:
✔ Leans CUT → ApoB >90 mg/dL + triglycerides >120 mg/dL + HDL <45 mg/dL + TG:HDL >2.0 + hs-CRP >2.0 mg/L. Any surplus is no longer partitioning efficiently. Nutrients are being stored as body fat while cardiometabolic risk increases.
✔ Leans BULK → ApoB <80 mg/dL + triglycerides <80 mg/dL + HDL >55 mg/dL + TG:HDL <1.5 + hs-CRP <1.0 mg/L. Metabolic optimal zone. Strong leptin/insulin sensitivity, low systemic inflammation, & adequate lipid transport. All make up conditions supporting productive lean mass gain.
✔ Common trap → Don’t get caught up over LDL-C. A mildly elevated LDL-C with low ApoB, low triglycerides, high HDL, and low hs-CRP is a much different phenotype than elevated LDL-C accompanied by high ApoB, rising triglycerides, and falling HDL. System of measures > single value.
Where do you get this all tested?
You can try ordering these 17 biomarkers at a normal physician’s office.
But not easily, anyway.
I found this out the hard way. I left my last annual physical with a $497 blood draw bill (still only tested 9 of these markers), two & a half hours of my life chewed up, and the stellar insight to stop taking creatine because of…elevated creatinine levels.
That’s the legacy system we’re working with. Built for average & allergic to root cause.
The other end of the spectrum isn’t better. Concierge medicine practices run for $10,000 to $40,000 per year. Great testing & services at unreasonable costs.
The gap here is why I’ve run Superpower for two years now. The highest ROI biomarker service built specifically for you — the elite practitioner.
➥ 100+ biomarkers in a single blood draw — all the above ones included
➥ One draw at any Quest location near you
➥ Results in 3 days
➥ 24/7 care team
➥ $199 a year
➥ HSA/FSA eligible
➥ Cancel anytime
And now, BTP readers get an additional 10% off through the link below.
You can’t dial in what you don’t measure. So start testing and stop guessing.
E. Recovery & Autonomic (Wearable-Derived)
Measures how your nervous system is adapting to training & catches an over-zealous deficit weeks in advance of other metrics.
Resting Heart Rate (RHR)
✔ Ideal target: <55 bpm
✔ Why it matters: Simplest & cheapest daily autonomic indicator of accumulated physiological stress. As recovery capacity diminishes, sympathetic activity rises, parasympathetic drive draws down, & RHR spikes before any noticeable performance hit.
✔ Reduce training volume / implement refeed if RHR drifts up 5–10 bpm above your baseline for days (deficit + training load outpacing recovery)
Heart Rate Variability (HRV)
✔ Ideal target: Highly relative metrics → stable or increasing relative to your rolling 30-day baseline. One of the worst measures to compare against the population…so don’t do it.
✔ Why it matters: Best marker of autonomic recovery → balance between sympathetic (”fight or flight”) & parasympathetic (”rest and digest”) nervous systems.
✔ Reduce training volume / increase calories / leverage deload week if HRV remains >10–20% below baseline for 3–5 consecutive days.
Sleep Architecture
✔ Ideal targets (in order of relative importance):
➜ Quality: Deep Sleep = 20–25%. REM = 20–30%.
➜ Efficiency: >85%
➜ Consistency: In bed by 10 PM → optimal GH bolus. Wake up ~sunrise.
➜ Duration: 6.5–9 hrs (highly bioindividual)
✔ Why it matters: Aggressive cuts will torch sleep (waking at 2–3 AM + overly active orexin signaling + hunger + chronically elevated cortisol baseline + low glycogen). Leads to poor follow on days of fuel partitioning and tissue repair.
✔ Stop cutting if deep/REM both fall off and you’re consistently waking through the night.
What this cluster tells you:
✔ Leans PAUSE CUTTING / BACK OFF → RHR up + HRV suppressed multi-day + sleep fragmenting. Execute a refeed, training pullback, or deficit pause.
✔ Leans ROOM TO PUSH → RHR and HRV stable to baseline + sleep / training recovery solid.
✔ Common trap → These metrics are only meaningful as a multi-day trend against your own baseline. Tracking the trend (relative to both YOU & TIME) > taking a snapshot in time.
Category 2: Unquantifiable Indicators
F. Drive & Libido
Dynamic behavioral expression of testosterone, estradiol, & central nervous system energy availability.
Morning Wood Frequency
✔ Baseline: Near-daily spontaneous morning erections.
✔ Why it matters: The canary in the cardiometabolic disease coal mine. A sensitive, leading signal of integrated androgen function, vascular status, nitric oxide signaling, & parasympathetic dominance during sleep.
✔ Stop cutting if frequency drops to absent for multiple consecutive days → signal of central energy conservation & early HPG-axis downregulation.
Spontaneous Libido
✔ Baseline: Consistent, unprovoked sex drive.
✔ Why it matters: Tracks blood flow + androgen signaling + estradiol sufficiency + dopaminergic sensitivity in real time. Often the first signal to decline under chronic energy deficit or high stress.
✔ Stop cutting if libido becomes absent despite adequate sleep or even consistent high UV conditions aren’t unlocking horniness → body signaling you have better things to worry about than your seed.
Drive & Initiative
✔ Baseline: Waking up with a fire that burns until the early evening.
✔ Why it matters: Reflects central dopaminergic tone & androgenic signaling in the brain. It’s less about sex hormones in isolation and more about behavioral output of the anabolic state.
✔ Stop cutting if persistently apathetic, passive, or avoidant → indicates systemic energy conservation overriding performance orientation.
G. Energy, Mood & Cognitive State
Real-time proxy for thyroid output, glucose stability, & allostatic load.
Thermal Regulation
✔ Baseline: Warm extremities & comfortable across moderate environments.
✔ Why it matters: Reflects thyroid-mediated metabolic rate & peripheral circulation. Decline a leading indicator to eventual reduced Free T3.
✔ Stop cutting if persistent cold intolerance (especially hands/feet) → metabolic downshift is occurring.
Afternoon Energy Stability
✔ Baseline: Steady intellectual horsepower & energy through 2–4 PM window.
✔ Why it matters: Valid test of glucose regulation & cortisol rhythm integrity. Energy crashes in the afternoon = early insulin sensitivity issues or deficit stress adding up.
✔ Stop cutting if consistent afternoon drained feeling & brain fog → clear sign of inadequate substrate availability. If body fat is elevated alongside slogging energy – allow it to be a signal to BEGIN a cut.
Mood Stability & Irritability Threshold
✔ Baseline: Emotionally stable in traffic or when someone is chewing loudly next to you.
✔ Why it matters: Reflects autonomic balance & cortisol reactivity. Energy deficits lower stress tolerance threshold.
✔ Stop cutting if irritability or emotional volatility hit new all-time highs every few days → allostatic load exceeding recovery capacity.
Cognitive Clarity
✔ Baseline: Easy to sustain focus for 60+ min.
✔ Why it matters: Since the brain is a high-energy demand organ, cognitive slowdown is an earlier signal of under-fueling before sh*t physical performance.
✔ Stop cutting if easily losing focus, no mental stamina, or dragging cognitively.
H. Training Felt-Sense
How neuromuscular output expresses when recovery, glycogen, & CNS readiness shift.
Logbook & Strength Perception (Grip / Load Feel)
✔ Baseline: Grip strength feels consistent & compound lifts are predictable relative to maintenance state.
✔ Why it matters: Logbook is the elite output metric. As CNS fatigue adds up, loads feel heavier & grip falls off before the logbook reflects.
✔ Implement a refeed if multiple sessions where normal working weights feel disproportionately heavy.
Pump & Muscular Fullness
✔ Baseline: Consistent fullness under training stimulus.
✔ Why it matters: Direct proxy for glycogen storage, intracellular hydration, & ideal insulin-mediated nutrient partitioning. An early sign of depleted glycogen stores.
✔ Stop cutting if not even high UV conditions + a high carb refeed day + 8g L-citrulline pre-workout can’t effectively counter flatness & loss of pump.
Joint, Tendon & Connective Tissue Recovery
✔ Baseline: Excellent mobility. No joint soreness. Minimal stiffness & quick recovery.
✔ Why it matters: Low energy availability + tanked E2 + overtraining stress amount to reduced collagen turnover & joint lubrication.
✔ Lower training volume if joints are achier than normal or tendons aren’t recovering well post-training.
I. Appetite, Hunger & Satiety Rhythms
Peripheral endocrine signaling of leptin, ghrelin, & central energy perception.
Satiety Response per Meal
✔ Baseline: Micronutrient-dense, high protein, high fiber meals satisfy for predictable duration.
✔ Why it matters: Satiety is the best qualitative proxy for effective leptin / insulin signaling, gastric emptying, & gut-brain feedback loop function.
✔ Stop cutting if even the most micronutrient dense meals fail to hit satiety cues.
Food Preoccupation
✔ Baseline: Food is contextual infrastructure for your daily performance & not dominating your frontal lobe.
✔ Why it matters: Increasing food salience reflects neuroendocrine adaptation to energy scarcity (dopaminergic reward reweighting).
✔ Stop cutting if food has become the mission. Living meal-to-meal with constant food thoughts dominating attention.
Hunger Intensity & Rhythms
✔ Baseline: Predictable & stable hunger rhythms throughout the day.
✔ Why it matters: Reflects leptin signaling integrity and hypothalamic energy sensing. True physiological hunger increases as energy availability drops (adaptive thermogenesis).
✔ Implement refeed if hunger becomes intrusive or sleep-disrupting daily → leptin is suppressed & the deficit reached an unsustainably high physiological tax.
None of these will be clear cut down the line.
Some will be wildly beneficial in determining your overall physiological state.
Some will be neutral conditions for you.
Some will be near useless for you.
Welcome to the story of the bioindividualized self.
Pay particular attention to daily rhythms.
Leverage the easy-to-measure, low hanging, high ROI signals.
Use blood biomarkers (hormonal + cardiometabolic) as often as possible.
A few additional resources I highly encourage you to leverage to support the path to your prime physique & an elite cardiometabolic condition:


Stay after it & until next time,
Phys