

More Isn't Better: The Case Against High-Dose Vitamin C
How a common supplement can accelerate the thing it's supposed to prevent

Cold coming on? Vitamin C.
Fortify your immune system? Vitamin C.
Improve redox balance status? Vitamin C.
Few ever question it.
But look past the reductionist marketing and the research tells a different story. One worth paying attention to if you’re taking even 500 mg per day.
Because among certain populations at certain doses, vitamin C supplements come with a cardiovascular cost.

The study that should change how you think about Vitamin C supplementation
In 2012, the Los Angeles Atherosclerosis Study (LAAS) tracked 573 healthy middle-aged adults aged 40–60 for a 3-yr period. The primary outcome measured was the carotid artery intima-media thickness (IMT). This is one of the most reliable early markers of atherosclerosis.
Researchers separated vitamin C intake into two categories: 1) from food sources & 2) from supplements.
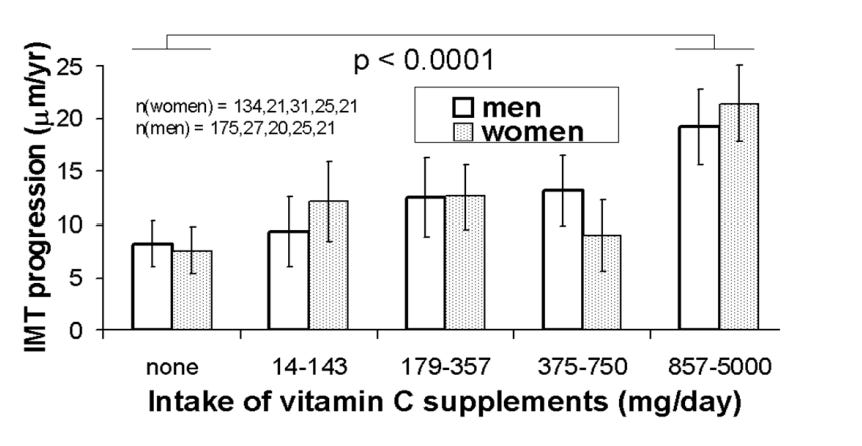
What they found was a nearly 3X FASTER arterial wall thickening in the highest supplement quartile.
People taking no vitamin C supplements saw IMT progression of 7.6 µm/year.
While those in the 857–5,000 mg/day range saw IMT progression of 20.3 µm/year.
And the dose-response was linear: more supplemental intake = more progression (p-trend = 0.0009).
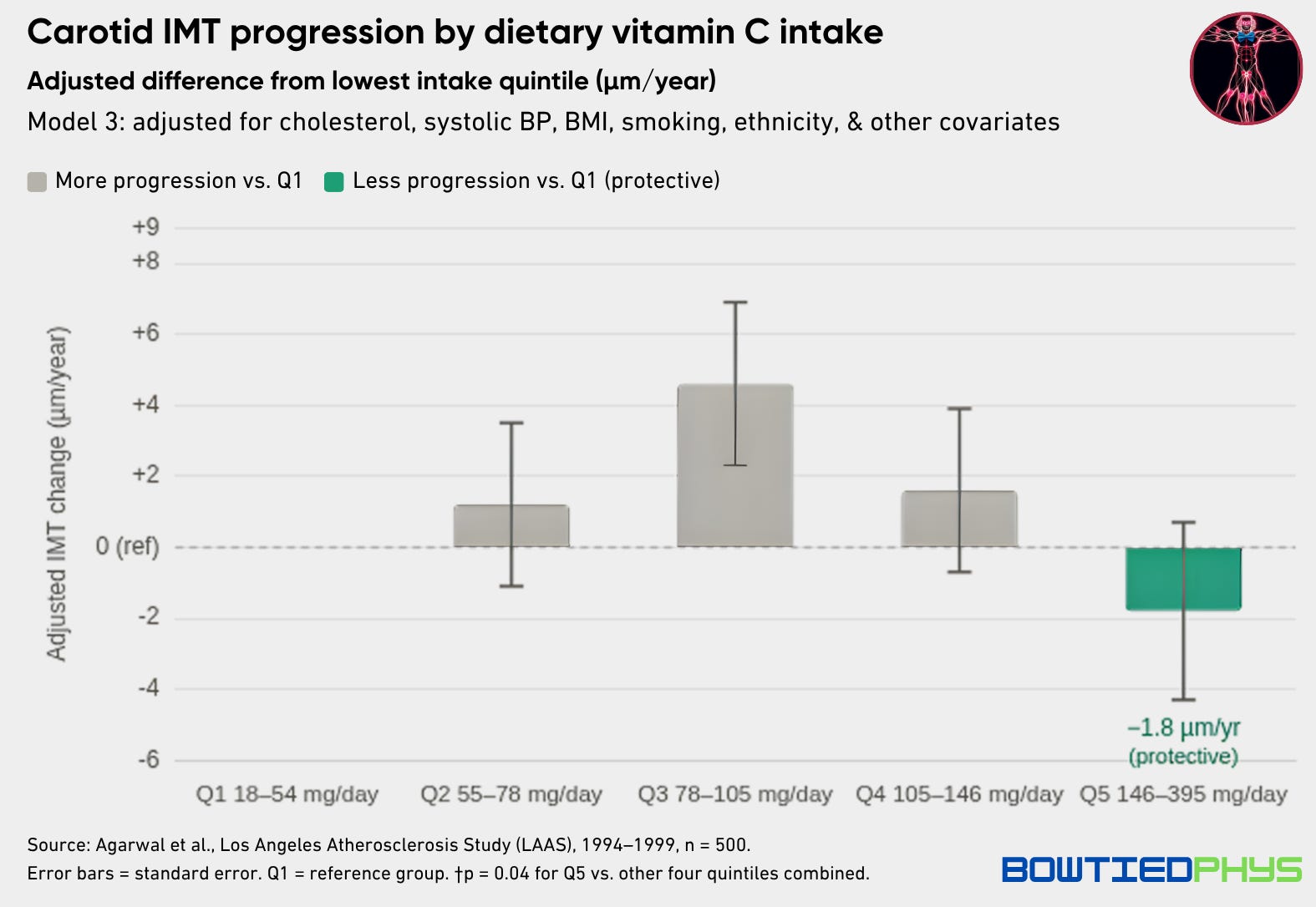
In the same study, vitamin C from food showed the opposite pattern.
The highest quintile of dietary vitamin C intake (~145–395 mg/day from actual whole food sources) was associated with less IMT progression (p = 0.008).
Some populations fare worse than others
The Iowa Women’s Health Study followed 1,923 postmenopausal women with diabetes for 15 years. After full adjustment for CVD risk factors, diabetes duration, & medications, women consuming ≥300 mg/day of vitamin C via supplements had significantly higher CVD & coronary artery disease mortality.
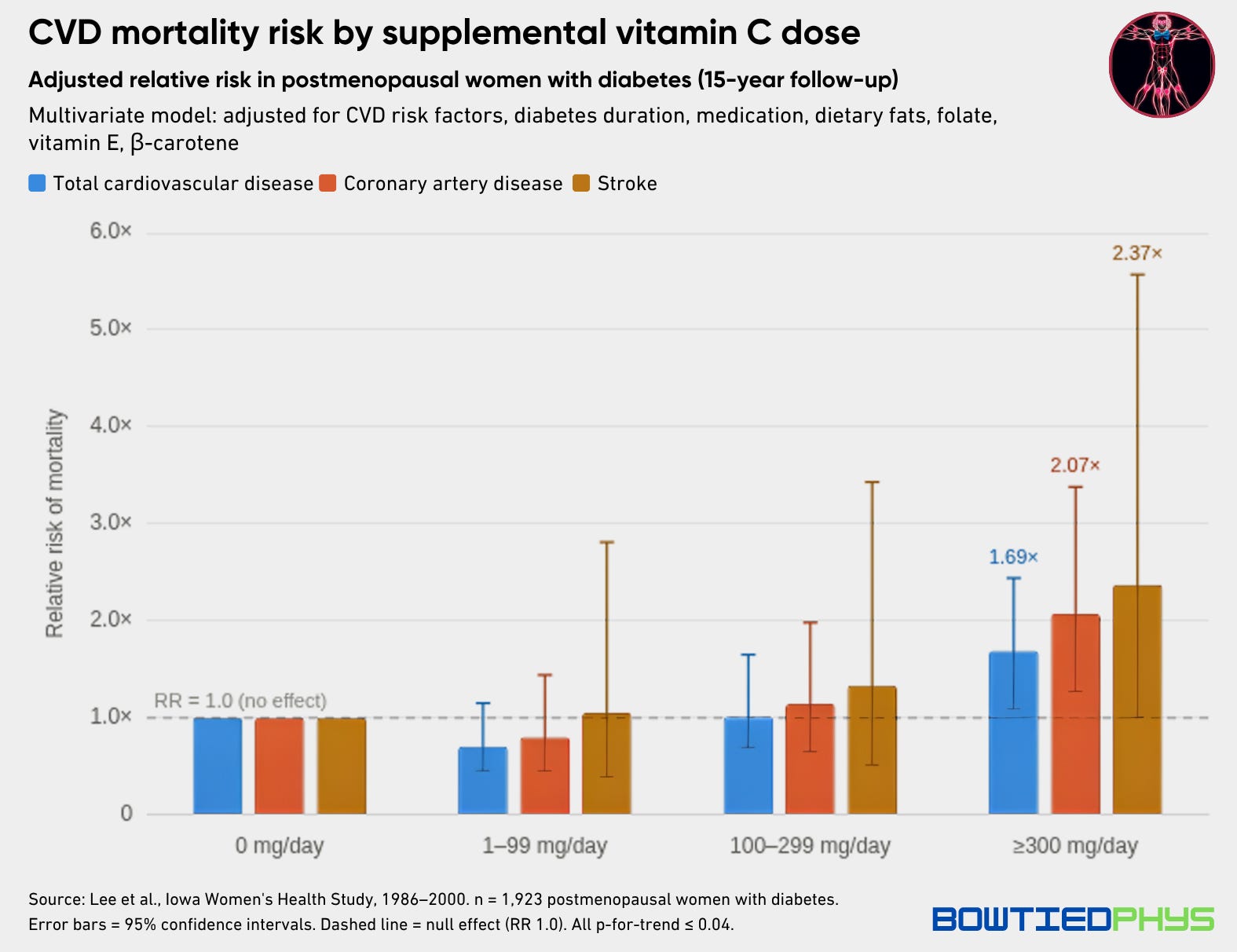
However worth noting — non-diabetic women from the same cohort had no association to increased CVD risk.
Two additional trials suggesting similarly:
In the WAVE trial, postmenopausal women with established coronary artery disease who took an antioxidant cocktail containing 1,000 mg vitamin C saw more coronary progression & higher all-cause mortality than placebo.
In the HATS trial, a similar antioxidant cocktail lowered HDL-C levels & blunted the lipid-lowering effects of statin + niacin therapy.
Why it happens
We know Vitamin C is a potent antioxidant. But at high intracellular concentrations, it shifts.
Vitamin C reduces Fe³⁺ to Fe²⁺ is what’s known as the Fenton reaction generating hydroxyl radicals & hydrogen peroxide.
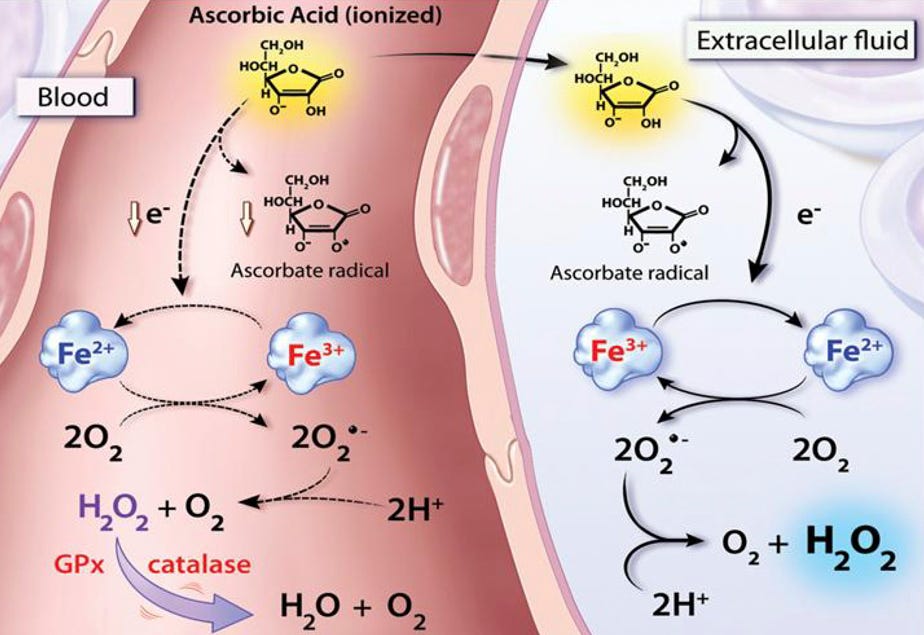
In a healthy, iron-regulated system, it’s not a major concern. But inside atherosclerotic plaques/or with metabolically diseased individuals, redox-active iron accumulates and this reaction becomes locally destructive.
Food-sourced vitamin C doesn’t reach concentrations high enough for free radical byproducts to pose an issue. It also gets packaged with flavonoids, carotenoids, & a redox-balanced matrix of cofactors that supplements cannot replicate. Yet another case of nature winning. Many such of these.
Balanced Approaches > Maxxing
Your takeaway shouldn’t be to become vitamin C avoidant. Quite the contrary.
In a 6-year RCT of hypercholesterolemic men & women (ASAP trial), moderate combined supplementation of vitamin E (136 IU) + slow-release vitamin C (250 mg) 2x daily slowed carotid IMT progression by ~25–26% vs. placebo (p = 0.014).
Ellingsen et al. (2009) also found that elderly men who increased fruit / vegetable intake by only ~80g/day (& subsequently vitamin C intake by ~13 mg/day) led to significantly less IMT progression over 3 years.
Food-sourced vitamin C / moderate supplementation > chronic high-dose supplementation
Practical Takeaways
1. Food first.
150–300 mg/day in a bioavailable, cofactor-rich form.

2. If needing to supplement, choose moderate doses of natural extracts over ascorbic acid supplements.
Acerola cherry. Camu camu. Kakadu plum. Rose hips.
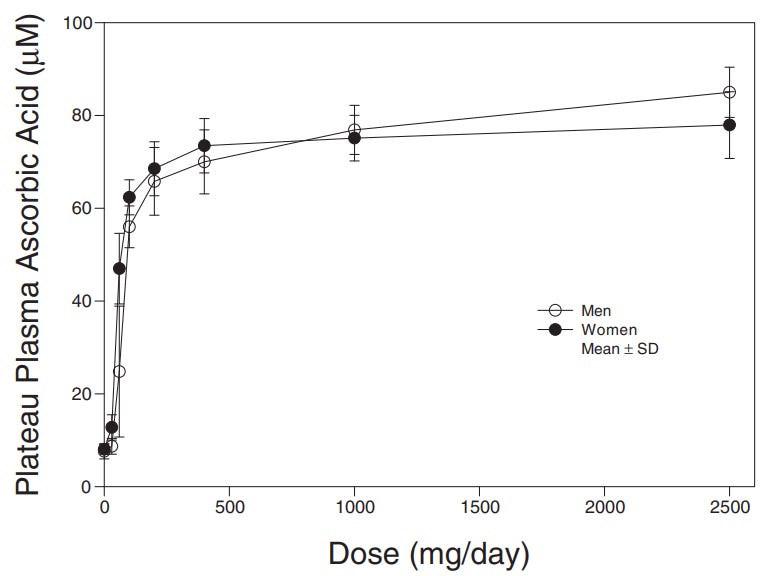
For most metabolically healthy men, ~400 mg/day vitamin C is the ceiling for chronic use. This saturates plasma without crossing into pro-oxidant territory.
Reserve 500–1,000 mg/day for an acute correction of seasonal sickness or documented deficiencies only. This can come in many forms. Once healthy again or levels normalize, drop back to food-first maintenance.
3. Let your biomarkers drive the decision.
Plasma ascorbate is what’s needed on bloodwork. Target 60–80 µmol/L where steady-state concentrations are met.
If you’re sitting in the mid-to-upper range from food alone, there’s very little evidence supporting additional supplementation.
Some adjacent markers to shape the full bioindividualized landscape:
hs-CRP: Elevated inflammatory load burns through antioxidant reserves faster. If CRP is chronically high, vitamin C turnover is higher and dietary intake needs to increase.
Ferritin & serum iron: High ferritin means more free iron available for the Fenton reaction. If ferritin is elevated (>200–300 ng/mL), high-dose vitamin C supplementation becomes unnecessarily risky.
Fasting glucose, fasting insulin, & HbA1c: A lack of metabolic flexibility & poor glucose metabolism amplifies vitamin C’s pro-oxidant potential and protein glycation effects.
Lipid panel (LDL-C, ApoB, oxLDL, Trig/HDL): The LAAS data showed the adverse effect of high-dose supplementation twice as much in those with elevated lipids in the top tertile.
4. Other factors influencing vitamin C status.
Several other factors increase vitamin C turnover and should influence how aggressively you’re going to prioritize intake:
➜ Training volume & intensity: High-volume endurance & intense resistance training increase the oxidative load. Match it to training load.
➜ Body composition: More lean mass increases high-ATP tissue demand.
➜ Heat exposure: Frequent sauna tips redox balance to an oxidative state and higher sweat-related micronutrient losses. Same goes with electrolyte losses.
➜ Excessive sunlight: UV radiation increases free radical production and subsequent antioxidant demand.
➜ High psychological stress loads: Cortisol & ascorbate compete for adrenal resources. Sustained stress via under-sleeping, overworking, & compounding life demands accelerates depletion.
➜ Age: Absorption efficiency declines and oxidative burden increases post-40.
➜ Restrictive diets: Carnivore. Keto. They will leave most functionally deficient.
➜ Acute illness: Immune activation depletes plasma levels. Needs will spike during infection, surgery, or recovery from injury.
If there’s anything that grinds my gears in the health space over the last year, it’s the “you need to be maxxing…” trend.

No. You shouldn’t be maxxing. Much more to come on this topic in the coming weeks.
For now, get your C from food.
Your friend,
Phys
Just so I undestand, 400mg is the recommendation for adult males?
Good to know, especially because these days all kinds of supplements come with added Vitamin C (collagen, electrolytes, etc.).